Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Definition and signs and symptoms of rhabdomyolysis
- Causes of rhabdomyolysis
- Treament and anesthetic management of rhabdomyolysis
Definition and mechanisms
- Rhabdomyolysis occurs when damaged skeletal muscle breaks down rapidly and releases its content in the bloodstream
- Characterized by skeletal muscle disintegration and the release of myoglobin and other intercellular proteins and electrolytes into the circulation
- Hyperkalemia, hyperuricemia, and hyperphosphatemia can all develop rapidly
- This can lead to heart- or kidney failure and can even be fatal
- Rhabdomyolysis ranges from an asymptomatic illness with elevation in the CK level to a life-threatening condition associated with extreme elevations in CK, electrolyte imbalances, acute kidney injury, and disseminated intravascular coagulation
- Most often caused by direct traumatic injury, however, can also result from a wide array of other causes
Signs and symptoms
- Muscle pains or cramps
- Weakness
- Swelling of affected muscles
- Nausea and vomiting
- Confusion
- Coma
- Tea-colored urine due to the presence of myoglobin
- Abdominal pain
- Fever
- Tachycardia
- Arrhythmias
- Hypotension and shock
- Acute kidney injury
AKI and rhabdomyolysis
- Myoglobin interacts with the Tamm-Horsfall protein in the renal tubules to form brown granular casts which lead to tubular obstruction
- This process is favoured when the urine is acidic
- The heme group of myoglobin could lead to lipid peroxidation
- Myoglobin also scavenges nitrous oxide leading to renal vasoconstriction
- Renal blood flow is furter reduced by hypovolemia, activation of the RAAS system and other vascular mediators
Complications
- Hyperkalemia
- Hypocalcemia
- Acute kidney injury
- Disseminated intravascular coagulation
- Compartment syndrome
Causes
- Strenuous exercise
- Delirium tremens
- Tetanus
- Prolonged seizures
- Crush injuries
- Arterial thrombosis or embolism
- Clamping of an artery during surgery
- Hyperthermia
- Hypothermia
- Drugs and toxins
- Statins and fibrates
- Antipsychotic medications may cause the neuroleptic malignant syndrome
- Neuromuscular blocking agents used in anesthesia may result in malignant hyperthermia, also associated with rhabdomyolysis
- Medications that cause serotonin syndrome, such as SSRIs
- Medications that interfere with potassium levels, such as diuretics
- Heavy metals
- Venom from insects or snakes
- Drugs: alcohol, amphetamine, cocaine, heroin, ketamine, and MDMA
- Infection
- Electrical injury
- Immobilization
- Metabolism:
- Hyperglycemic hyperosmolar state
- Hyper– and hyponatremiamia
- Hypokalemia
- Hypocalcemia
- Hypophosphatemia
- Ketoacidosis
- Hypothyroidism
Risk factors
| Endogenous Risks | Exogenous Risks |
|---|---|
| Advanced age (> 80 years) Small body frame and frailty Multisystem disease - Renal dysfunction - Hepatic dysfunction Thyroid disorders, especially Hypothyroidism Hypertriglyceridemia Metabolic muscle disease - Carnitine palmitoyltransferase II deficiency - McArdle disease Myoadenylate deaminase deficiency | Alcohol consumption Heavy exercise Surgery with severe metabolic demands Agents affecting the cytochrome P450 system, especially - Fibrates - Nicotinic acid - Cyclosporine - Azole antifungals - Macrolide antibiotics - HIV protease inhibitors - Nefazodone - Verapamil - Amiodarone - Warfarin - Consumption of > 1 quart daily of grapefruit juice |
Diagnosis
- Blood test: creatine kinase (CK) > 5000 U/L
- Note that myoglobin levels peak before increases in CK
- However, myoglobin is metabolized rapidly at sites outside of the kidney
- This makes CK a more reliable marker of rhabdomyolysis
| Investigations | Possible findings |
|---|---|
| Serum and urine myoglobin | Present |
| Urinary dipstick + pH | Positive for blood |
| Urea and creatinine | Raised |
| Potassium | Raised |
| Calcium | Low |
| Phosphate, uric acid | Raised |
| Coagulation studies | Prologend in severe cases |
| Blood gas | Lactic acidosis |
| Calculation of anion gap | Raised |
| ECG | Prologend in severe cases |
- A metabolic acidosis with a high anion gap is commonly reported in rhabdomyolysis with associated AKI
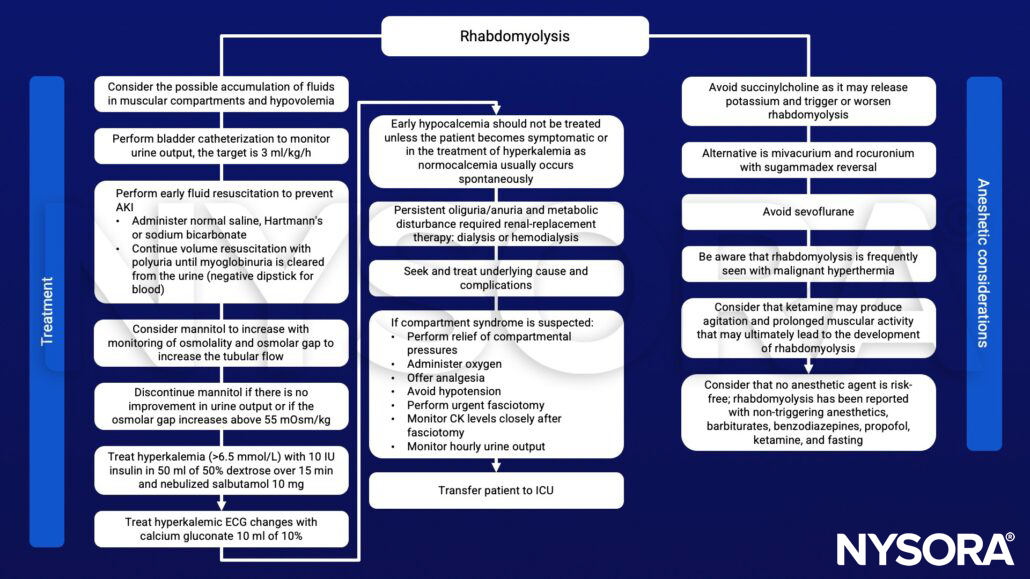
Management
Suggested reading
- Floridis, J., Barbour, R., 2022. Postoperative weakness and anesthetic-associated rhabdomyolysis in a pediatric patient: a case report and review of the literature. Journal of Medical Case Reports 16.
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Torres PA, Helmstetter JA, Kaye AM, Kaye AD. Rhabdomyolysis: pathogenesis, diagnosis, and treatment. Ochsner J. 2015;15(1):58-69.
- Williams J, Thrope C. 2014. Rhabdomyolysis. Continuing Education in Anaesthesia Critical Care & Pain. 14;4:163-166.
- Hunter JD, Greggg K, Damani S. 2006. Rhabdomyolysis. Continuing Education in Anaesthesia Critical Care. 6;4:141-143.