- Learn
-
Apps
View all apps
Veterinary
 VetRA App
VetRA App

- Books
- Events
- News
- Partners
- About
- For Clinicians
 VetRA App
VetRA App

Where Anesthesiology Is Learned, Practiced, and Advanced





We train clinicians, influence practice and scale innovation.
Our Track Record
Annual Visitors
Clinicians Reached
Newsletter Subscribers
Industry Partners
Discover expert content, clinical guidance, and practical learning resources.
Anesthesiology
Explore critical topics, techniques, and anesthesia trends.
Read Articles
Regional Anesthesia
Step-by-step guides, nerve blocks, and clinical best practices.
Read Articles
Pain Management
Access interventional techniques and real-life case studies.
Read Articles
IV Access
Master routine and challenging IV access with practical tips.
Read Articles
POCUS
The most widely used point-of-care ultrasound techniques for rapid bedside assessment.
Read Articles

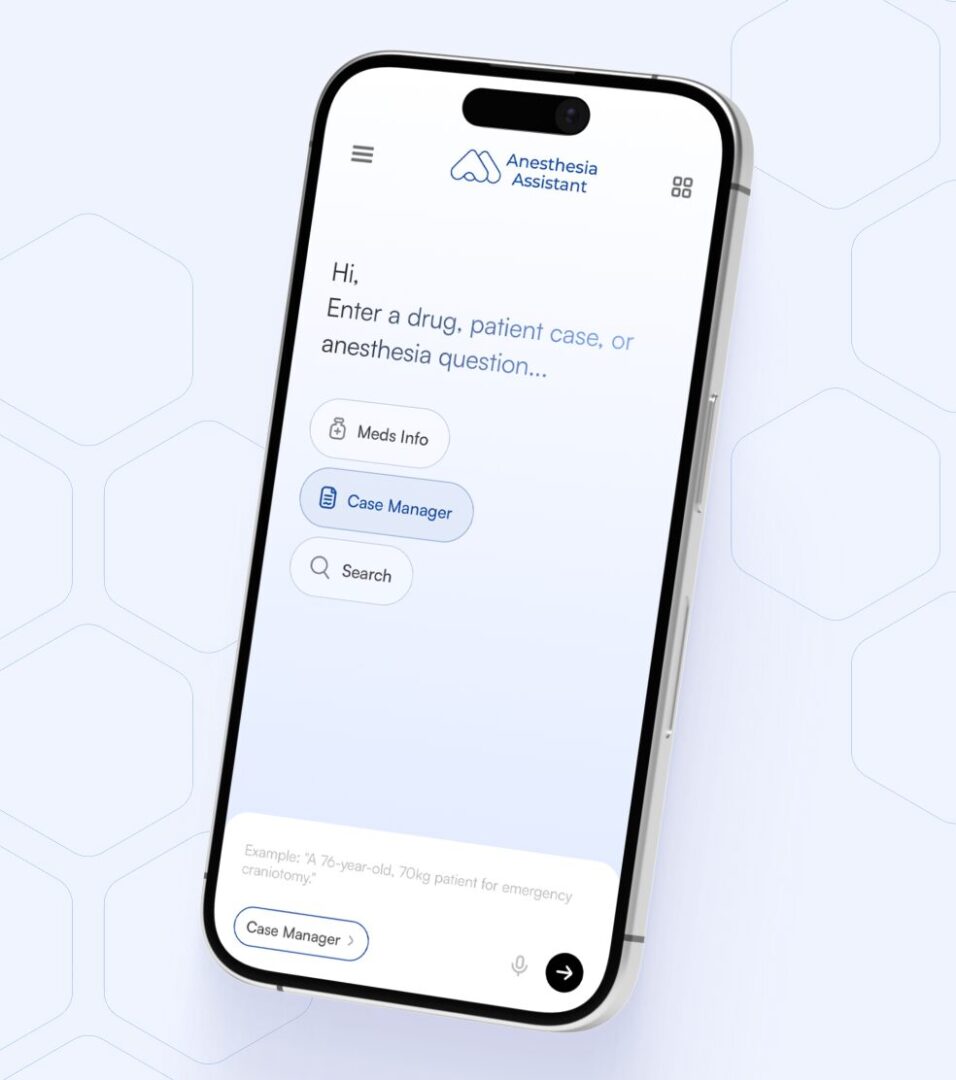
Case management. Medication guidance. Anesthesia-relevant search - all in one place. Trusted by anesthesiologists worldwide.


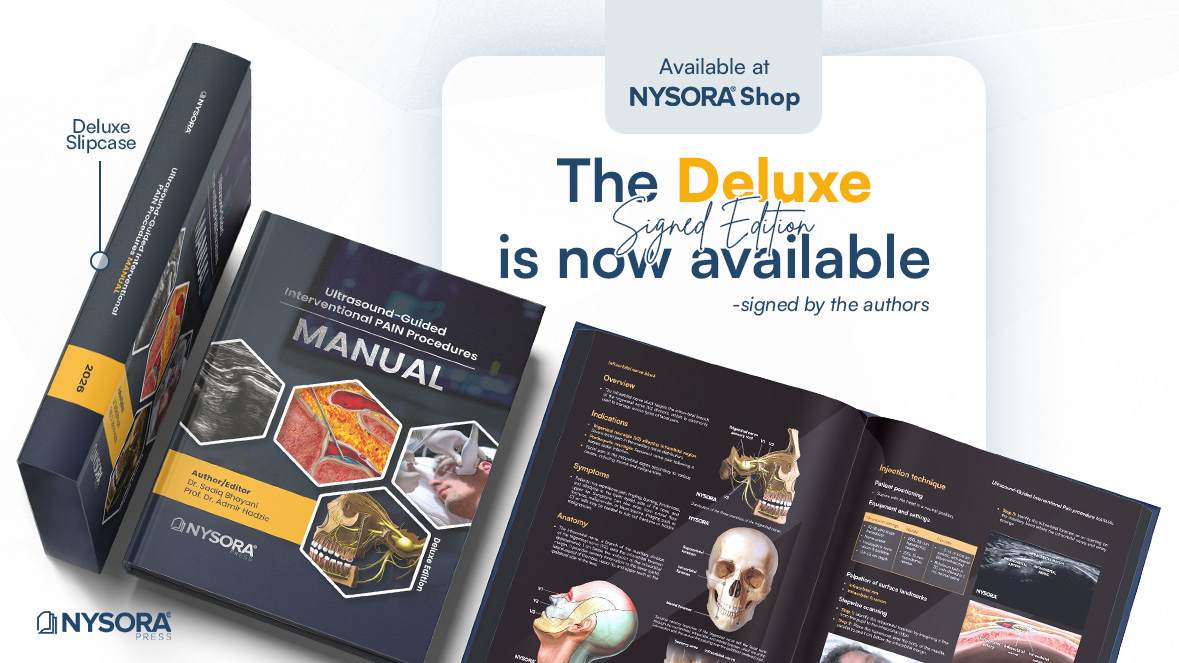
A comprehensive, step-by-step guide covering pain procedures across all anatomical regions.
Deluxe version is now available.

Beyond Simulation - Train Where Regional Anesthesia Happens
Practical anesthesia knowledge you can apply in your next case-delivered straight to your inbox.


















Expand your expertise through NYSORA’s CME-accredited events. Join anesthesiologists and pain specialists worldwide for live training, case discussions, and professional networking.

Update on Regional Anesthesia and Pain Management

Anesthesia Review Conference

Regional Anesthesia Conference

Regional Anesthesia Conference

Regional Anesthesia Conference

Ultrasound-Guided Regional Anesthesia Boutique Workshop

Ultrasound-Guided Regional Anesthesia Boutique Workshop

Ultrasound-Guided Regional Anesthesia Boutique Workshop

Ultrasound-Guided Regional Anesthesia Boutique Workshop

Pediatric Regional Anesthesia Boutique Workshop

Ultrasound-Guided Regional Anesthesia Boutique Workshop

Ultrasound-Guided Regional Anesthesia Boutique Workshop

Ultrasound-Guided Regional Anesthesia Boutique Workshop

Ultrasound-Guided Regional Anesthesia Boutique Workshop

Ultrasound-Guided Regional Anesthesia Boutique Workshop
Point Of Care Ultrasound (POCUS) Workshop

Ultrasound in Interventional Pain Medicine Comprehensive Workshop (Plus CIPS Exam preparation Instructions)
Ultrasound-Guided Regional Anesthesia Boutique Workshop

Ultrasound-Guided Regional Anesthesia Boutique Workshop
Orthobiologics Workshop for MSK and Spine
Ultrasound-Guided Regional Anesthesia Boutique Workshop

Ultrasound-Guided Regional Anesthesia Boutique Workshop
Ultrasound-Guided Regional Anesthesia Boutique Workshop

Regional Anesthesia Boot Camp

Regional Anesthesia Boot Camp

Regional Anesthesia Boot Camp

Regional Anesthesia Boot Camp
Regional Anesthesia Boot Camp

Regional Anesthesia Boot Camp

Regional Anesthesia Boot Camp

Regional Anesthesia Boot Camp

Regional Anesthesia Boot Camp

Regional Anesthesia Boot Camp

Regional Anesthesia Boot Camp

Regional Anesthesia Boot Camp

Regional Anesthesia Boot Camp
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About