Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About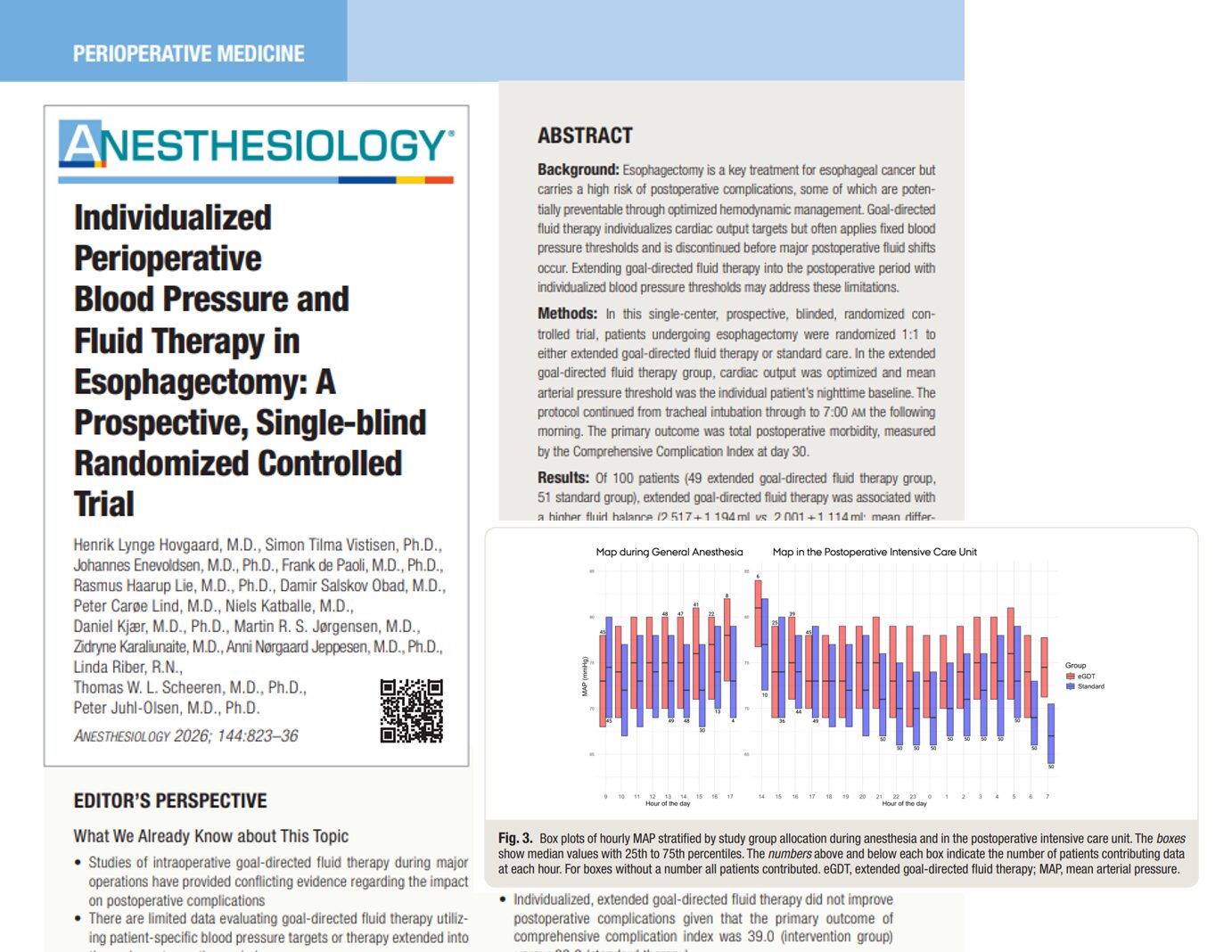





Major thoracic surgery, particularly esophagectomy, carries a substantial risk of postoperative morbidity. Clinicians have long explored goal-directed fluid therapy (GDT) and hemodynamic optimization as strategies to improve outcomes.
A new randomized controlled trial published in Anesthesiology (2026) challenges this paradigm, showing that even highly individualized perioperative blood pressure and fluid strategies may not reduce complications.
Overview of the study
This prospective, single-blind randomized controlled trial evaluated whether extending individualized hemodynamic management beyond surgery improves outcomes.
Study design
- Population: 100 patients undergoing esophagectomy
- Intervention:
- Extended goal-directed fluid therapy (eGDT)
- Individualized mean arterial pressure (MAP) targets based on preoperative nighttime blood pressure
- Control: Standard hemodynamic care
- Duration of intervention: From anesthesia induction to the first postoperative morning
Primary outcome
- Comprehensive complication index (CCI) at 30 days
Key findings
No reduction in complications
- CCI score:
- eGDT: 39.0 ± 20.0
- Standard care: 39.2 ± 21.0
- No statistically or clinically significant difference
Increased intervention without benefit
Patients in the individualized group experienced:
- Higher fluid administration
- Increased norepinephrine use
- Slightly higher mean arterial pressure
Despite these changes:
- No improvement in postoperative morbidity
- No difference in hospital or ICU length of stay
Complication burden remained high
- 98% of patients in the intervention group had at least one complication
- 96% in standard care
- Over 460 complications recorded at 30 days
What is goal-directed fluid therapy?
Goal-directed fluid therapy (GDT) aims to optimize:
- Cardiac output
- Tissue perfusion
- Oxygen delivery
Traditional approach
- Uses dynamic parameters such as:
- Stroke volume variation (SVV)
- Cardiac output monitoring
- Often applies fixed MAP thresholds (e.g., ≥65 mmHg)
What makes this study different?
This trial introduced two key innovations:
-
Individualized blood pressure targets
- MAP targets derived from each patient’s baseline nighttime blood pressure
- Range typically between 65–85 mmHg
-
Extended therapy into postoperative period
- Continued hemodynamic optimization until the morning after surgery
- Addresses:
- Fluid shifts
- ICU hemodynamic instability
Why didn’t individualized therapy improve outcomes?
-
Minimal hemodynamic separation
- Actual MAP difference between groups: ~3 mmHg
- Clinically insignificant despite different targets
-
Macro vs microcirculation mismatch
Optimizing global parameters (MAP, cardiac output) does not guarantee:
- Adequate microvascular perfusion
- Tissue oxygenation
-
Improved standard care
Modern perioperative care already includes:
- Careful fluid management
- Real-time hemodynamic assessment
- Reduced variability in practice
This may reduce the added benefit of protocolized GDT.
-
Physiological complexity after surgery
Postoperative changes include:
- Increased oxygen demand after extubation
- Altered cardiac loading conditions
- Dynamic fluid redistribution
These factors may limit the effectiveness of fixed protocols.
Clinical implications
What this means for anesthesiologists
- Routine use of extended, individualized GDT may not be justified
- Focus should shift toward:
- Clinical judgment
- Dynamic reassessment
- Avoiding fluid overload
Important considerations
- Overuse of vasopressors and fluids may:
- Increase complications
- Add unnecessary complexity
Conclusion
This landmark trial provides important clarity:
- Individualized blood pressure and fluid therapy did not improve outcomes after esophagectomy
- Increased intervention intensity did not translate into clinical benefit
- The role of goal-directed therapy is being re-evaluated in modern perioperative care
The future likely lies not in more aggressive hemodynamic manipulation, but in better understanding tissue-level physiology and individualized patient response.
Reference: Hovgaard HL et al. Individualized Perioperative Blood Pressure and Fluid Therapy in Esophagectomy: A Prospective, Single-blind Randomized Controlled Trial. Anesthesiology. 2026;144:823-836.
Explore more about the management of esophagectomy patients in NYSORA’s Anesthesiology Manual. And for a digital learning experience, check out the Anesthesiology Module on NYSORA360!