
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the risk factors for malignant hyperthermia
- Describe the symptoms of malignant hyperthermia
- Manage malignant hyperthermia and its consequences
Definition & mechanism
- Malignant hyperthermia (MH) is caused by genetic defects, most commonly in the RYR1 gene (more rarely affected genes include CACNA1S and STAC3)
- Caused by an increase in metabolic rate driven by an increase in intracellular calcium levels in muscle tissue
- Can be triggered when exposed to potent inhalation anesthetics and/or succinylcholine
Risk factors
Patients that have a higher risk of MH when exposed to triggering agents:
- Any close relative has a confirmed susceptibility to MH
- The patient or a close relative has a history of an event that is suspected to be MH during anesthesia
- The patient or a close relative has a history of rhabdomyolysis, which can be triggered by exercise in extreme heat and humidity or when taking a statin drug
- Patients with another genetic muscle disorder (e.g. Duchenne muscular dystrophy)
- Patients with idiopathic hyperCKemia
- Patients with otherwise unexplained exertional heat illness
Symptoms
- Unexplained, unexpected increase in ETCO2
- Unexplained, unexpected increase in heart rate
- Unexplained, unexpected increase in temperature
- Decreased urine output
- Muscle spasms
- Masseter muscle rigidity
Management
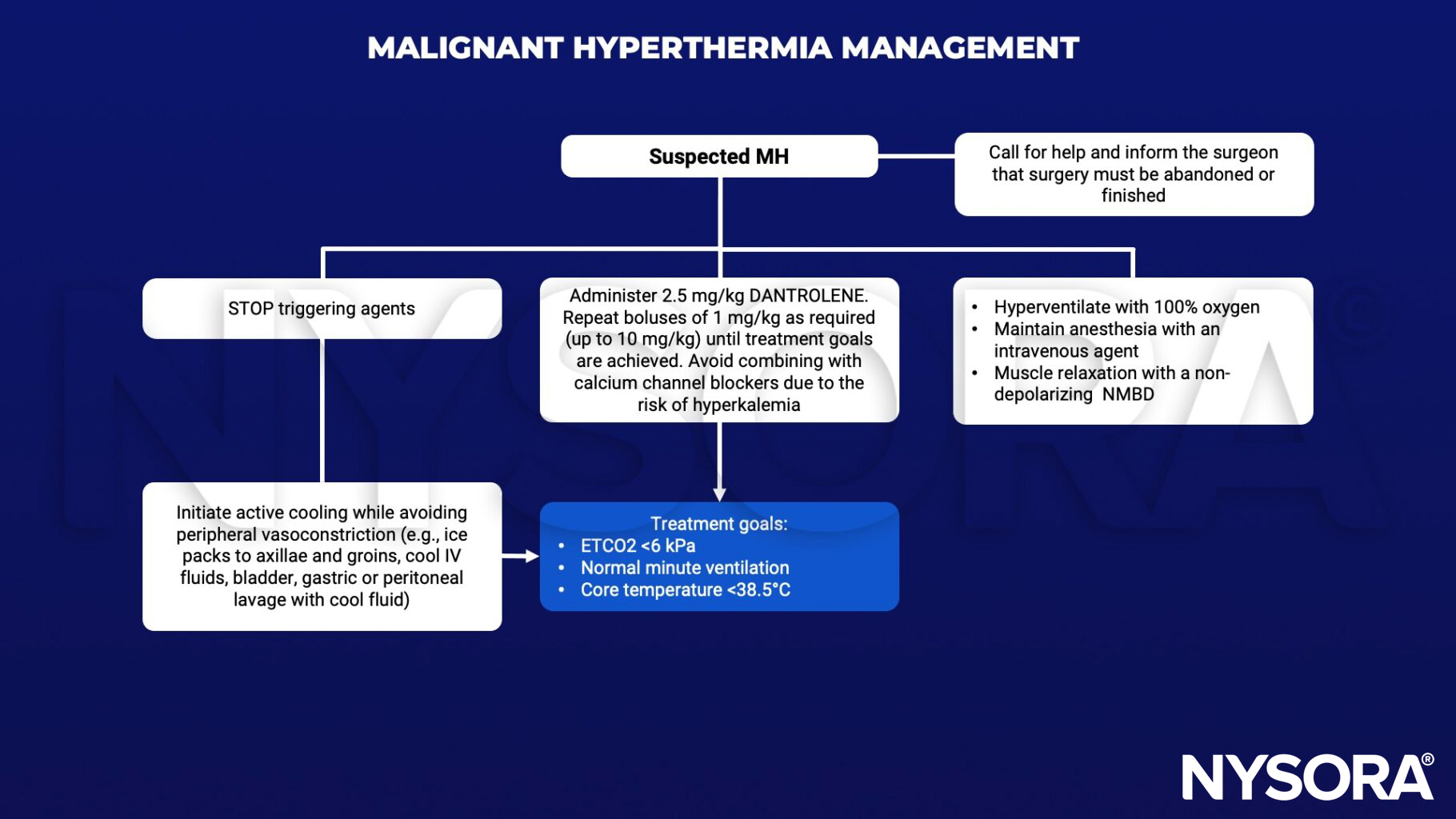
Supportive management
- Hyperkalemia may require administration of calcium chloride, sodium bicarbonate, and/ or insulin with glucose
- Treat arrhythmias with magnesium, amiodarone or beta-blockers. Avoid calcium channel blockers as they interact with dantrolene, potentiating myocardial depression
- Disseminated intravascular coagulation may require blood product transfusion
- Rhabdomyolysis may result in acute kidney injury; measure creatine kinase and institute forced alkaline diuresis
- Transfer the patient to the ICU once sufficiently stable
Follow-up:
- The diagnosis of MH is confirmed by muscle biopsy and in vivo contracture testing at specialist centers
- The patient and their family members must be followed-up and counseled regarding future anesthetics
- An alert should be documented in the patient notes and the patient should consider wearing an alert bracelet or carrying an alert card to notify medical staff of their condition in case of future emergencies
Keep in mind
- Taking a personal and family history of anesthetic problems is a mandatory part of the preoperative assessment for all patients requiring general or regional anesthesia
- Activated charcoal filters should be available at all anesthetizing locations
- Patients at increased risk of developing malignant hyperthermia must not be exposed to potent inhalation anesthetics or succinylcholine
Suggested reading
- Hopkins PM, Girard T, Dalay S, et al. Malignant hyperthermia 2020: Guideline from the Association of Anaesthetists. Anaesthesia. 2021;76(5):655-664.
- Gupta, Pawan K, and Philip M Hopkins. “Diagnosis and Management of Malignant Hyperthermia.” BJA Education, vol. 17, no. 7, July 2017, pp. 249–254, 10.1093/bjaed/mkw079.
Clinical updates
Glahn et al. (2025, BJA) publish updated European Malignant Hyperthermia Group (EMHG) guidelines emphasizing earlier recognition based on rising ETCO₂ and metabolic acidosis, immediate cessation of triggering agents, and prompt, repeated dosing of dantrolene (2–2.5 mg/kg IV, up to ≥ 10 mg/kg total). New recommendations include routine use of activated charcoal filters, clearer algorithms for hyperkalemia and cooling, and mandatory 24-hour ICU-level monitoring due to recurrence risk.
- Read more about this study HERE.
Rüffert et al. (2026, BJA) present updated EMHG guidelines for investigating malignant hyperthermia susceptibility, introducing the new MH genotype (MHG) classification for individuals with pathogenic or likely pathogenic variants (e.g. RYR1, CACNA1S) even without confirmatory IVCT. The guidelines integrate genetic testing as the first-line investigation in patients with personal or family MH history, while reaffirming in vitro contracture testing (IVCT) as the only method to definitively exclude MH risk.
- Read more about this HERE.











