Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Definition and types of scoliosis
- Non-operative treatment options
- Pre-operative evaluation
Definition and mechanisms
- Scoliosis refers to lateral curvature of the spine, vertebral body rotation, and angulation of the rib
- These are classified as structural or non-structural (e.g. length discrepancy)
- Men and women are equally affected with women often requiring more surgical intervention
- Congenital scoliosis:
- May present at any age and is a result of either failure of vertebral segmentation (a bar) or failure of formation (a hemivertebra)
- Congenital scoliosis is often part of a generalized condition, such as Goldenhar syndrome or spina bifida
- It may be associated with abnormalities in renal, cardiac, respiratory, or neurological systems
- Acquired scoliosis:
- Mainly idiopathic
- Infantile onset idiopathic scoliosis (scoliosis before the age of 8 years) carries the most serious prognosis and if left unchecked is likely to result in cardiopulmonary failure in middle age
Types of scoliosis
| Idiopathic scoliosis is the most common with a wide range of causes | Collagen abnormalities, hormones, genetics, and growth abnormalities |
| Neuromuscular | Neuropathic Upper motor neuron (e.g. cerebral palsy, spinal cord injury) Lower motor neuron (poliomyelitis, myelomeningocele, spinal muscular atrophy) Familial dysautonomia |
| Myopathic | Muscular dystrophy Myotonic dystrophy |
| Congenital | Hemivertebrae Congenitally fused ribs |
| Neurofibromatosis | Marfan’s syndrome Osteogenesis imperfecta Arthrogryposis |
| Trauma | Vertebral fracture or surgery Post thoracoplasty Post radiation |
Neuromuscular scoliosis has been associated with increased intraoperative blood loss compared with idiopathic scoliosis
Diagnosis
- X-ray
- Clinical examinations
Classification of severity
- Cobb Angle:
- Measured from a standing anteroposterior radiograph of the spine
- The surgical treatment is recommended if the cobb angle is greater than 45° – 50°
- Degree of Cobb Angle associated with pulmonary and cardiovascular dysfunction
Conditions associated with scoliosis
- Decreased overall lung function (restrictive) with significantly reduced vital capacity and respiratory muscle function can be impaired as well
- An increased pulmonary vascular resistance and pulmonary hypertension, possibly leading to right ventricle hypertrophy and failure
- Increased risk of mitral valve prolapse
- Increased risk for malignant hyperthermia if scoliosis results from muscular dystrophies
- Potential difficult airway
Non-operative treatment
- Rigid bracing (thoracolumbosacral orthosis)
- Indicated for a progressive curve greater than 25°
- Results depend on compliance (social stigma and discomfort)
- Serial full-body casting
- Indicated for infantile scoliosis
- General anesthesia is required every 2-3 months
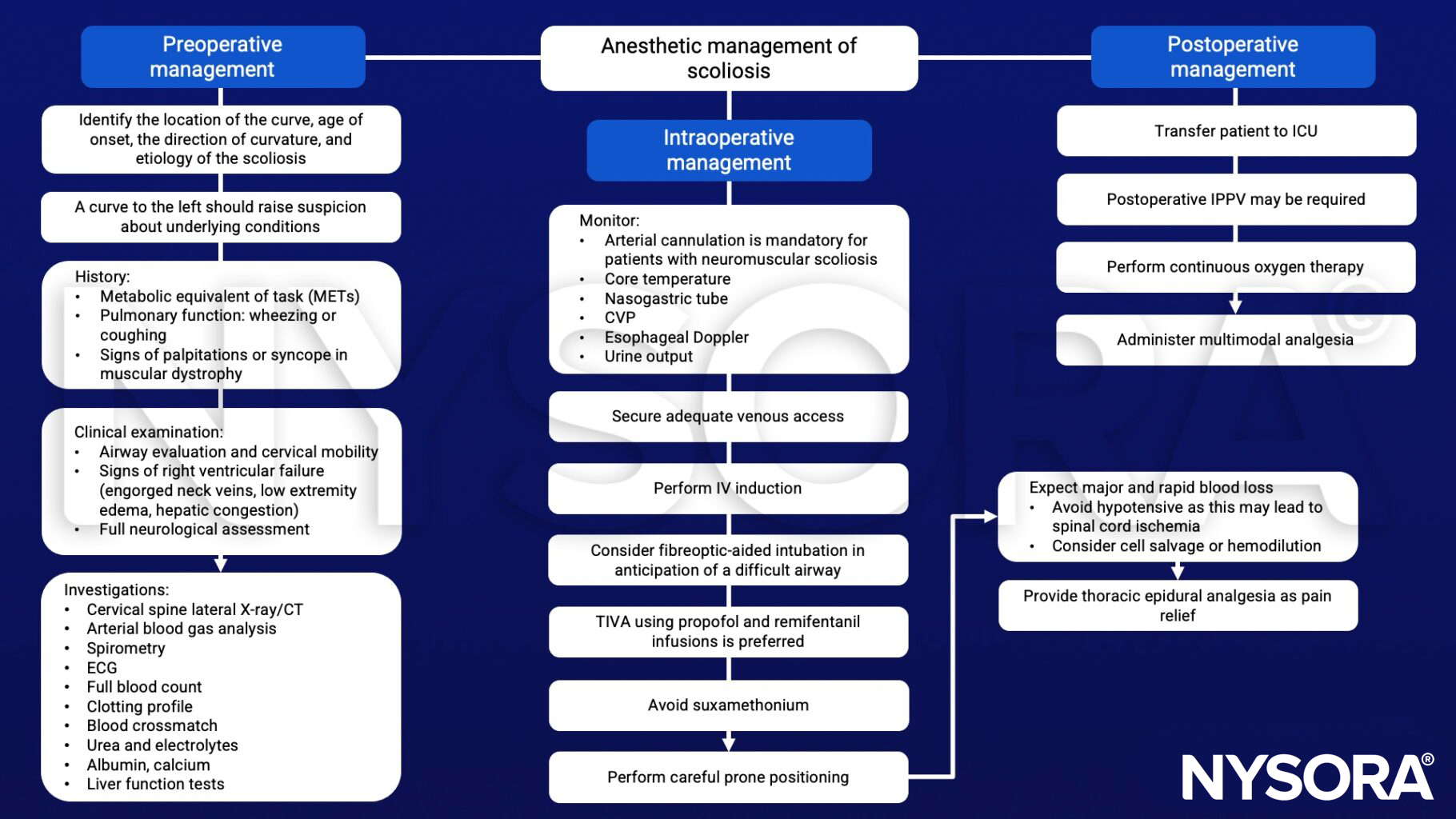
Management
See also spine surgery
Suggested reading
- Yao FS, Hemmings HC, Malhotra V, Fong J. 2021. Yao & Artusio’s Anesthesiology: Problem-Oriented Patient Management. Chapter 58 – scoliosis (9th edition). Wolters Kluwer Health/Lippincott Williams & Wilkins.
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Gadsden, J., & Jones, D. (2011). Anesthesiology Oral Board Flash Cards. McGraw-Hill Education.
- Gambrall MA. Anesthetic implications for surgical correction of scoliosis. AANA J. 2007;75(4):277-285.
Clinical updates
Choi et al. (Regional Anesthesia & Pain Medicine, 2024) demonstrate that in children with thoracolumbar scoliosis, ultrasound estimation of epidural depth using the paramedian sagittal oblique (PSO) view correlates more accurately with actual epidural depth than the transverse median view and provides superior visualization of neuraxial structures.