Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Definition, diagnosis, and management of hypernatremia
Definition
- Serum sodium > 145 mmol/L
- Severe symptoms usually occur at concentrations > 160 mmol/L
Signs and symptoms
| Mild symptoms | Severe symptoms |
|---|---|
| Anorexia Muscle weakness Restlessness Headache Confusion Nausea | Vomiting Seizures Coma Brain shrinkage, resulting in vascular rupture and intracranial bleeding |
Causes
- Decreased intake or increased loss of water resulting in a net loss in water
- Increase in sodium intake as a cause is rare
| Primary hypodipsia | Lack of thirst Usually caused by destruction of the hypothalamic thirst center Due to primary or metastatic tumors, granulomatous disease, vascular disease or trauma |
| Diabetes insipidus | Caused by a defect in the secretion of ADH in the hypothalamus or by a defective response to ADH in the renal tubules Resulting in production of large amounts of urine (polyuria), thereby raisings the Na+ |
| Pure hypertonic saline gain | Relatively rare cause of hypernatremia caused by the ingestion of hypertonic solutions |
| Combination of inadequate fluid intake + increased free water loss | The most common cause of hypernatremia in the elderly Pathophysiology: the thirst mechanism weakens and renal function declines with increasing age Frail elderly people, particularly those living alone may also have difficulties obtaining adequate fluid volumes |
| Hyperglycemia | |
| Hyperaldosteronism |
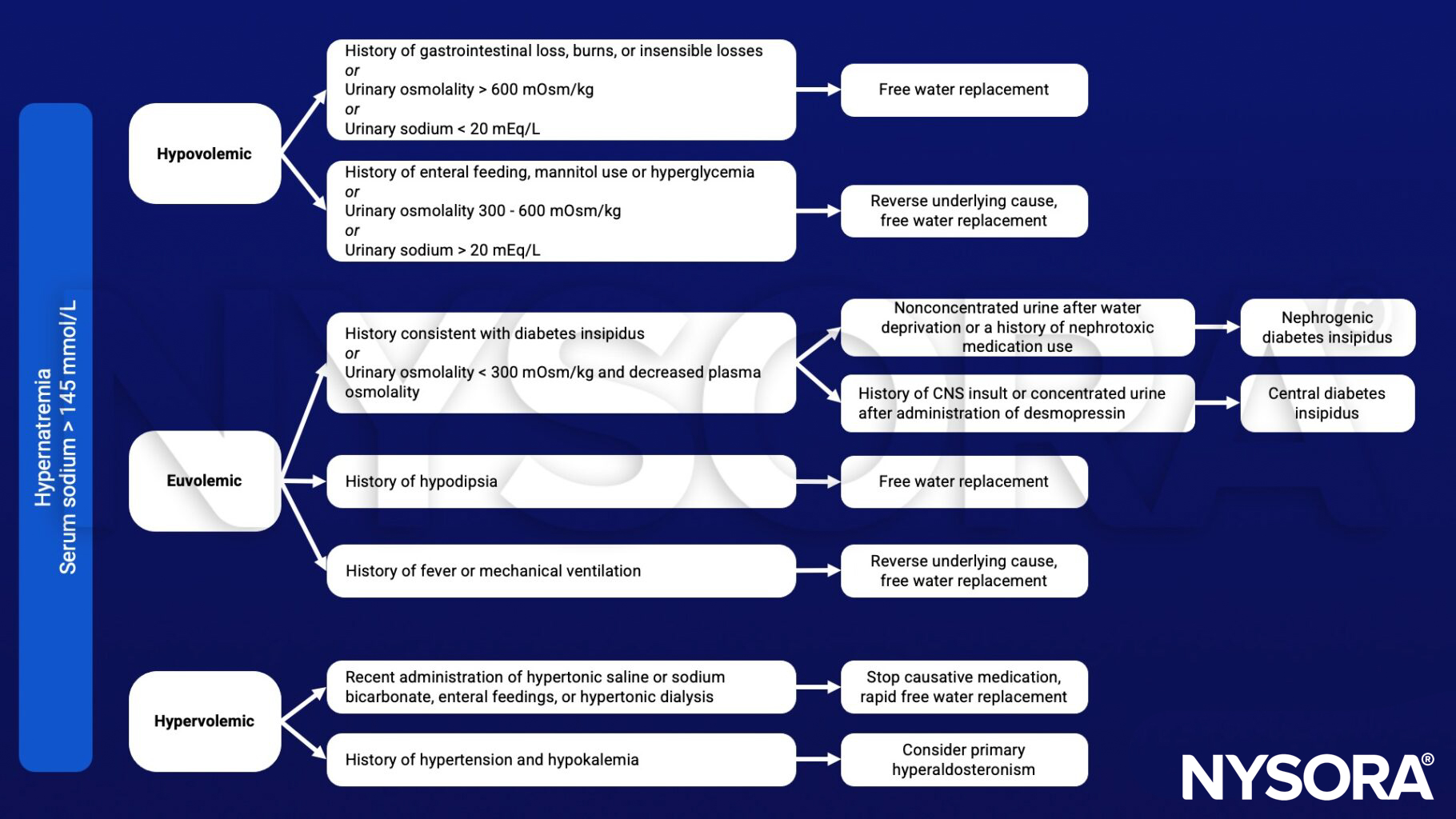
Management
- Estimate volume status and total body water deficit with this formula: WD1 = 0.6 × bodymass × [1 − (140 ÷ Na+)]
- Treat the underlying cause and correct the water deficit
- First choice of fluid: oral free water
- IV: use hypotonic solutions
- Do NOT rapidly correct or overcorrect, this increases the risk for cerebral edema
- A correction rate of 1 mmol/L per hour is considered a safe rate of correction
- NOTE: This rate is NOT recommended in chronic hypernatremia!
- In patients where hypernatremia is present for a longer period, the sodium level should be corrected at a rate of 0.5 mmol/L per hour, max 8 – 10 mmol/L per 24 hours
- In patients with acute hypernatremia, quick correction of sodium can be perfomed safely with isotonic saline or water without the risk of cerebral edema
Suggested reading
- Braun MM, Barstow CH, Pyzocha NJ. Diagnosis and management of sodium disorders: hyponatremia and hypernatremia. Am Fam Physician. 2015;91(5):299-307.