Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About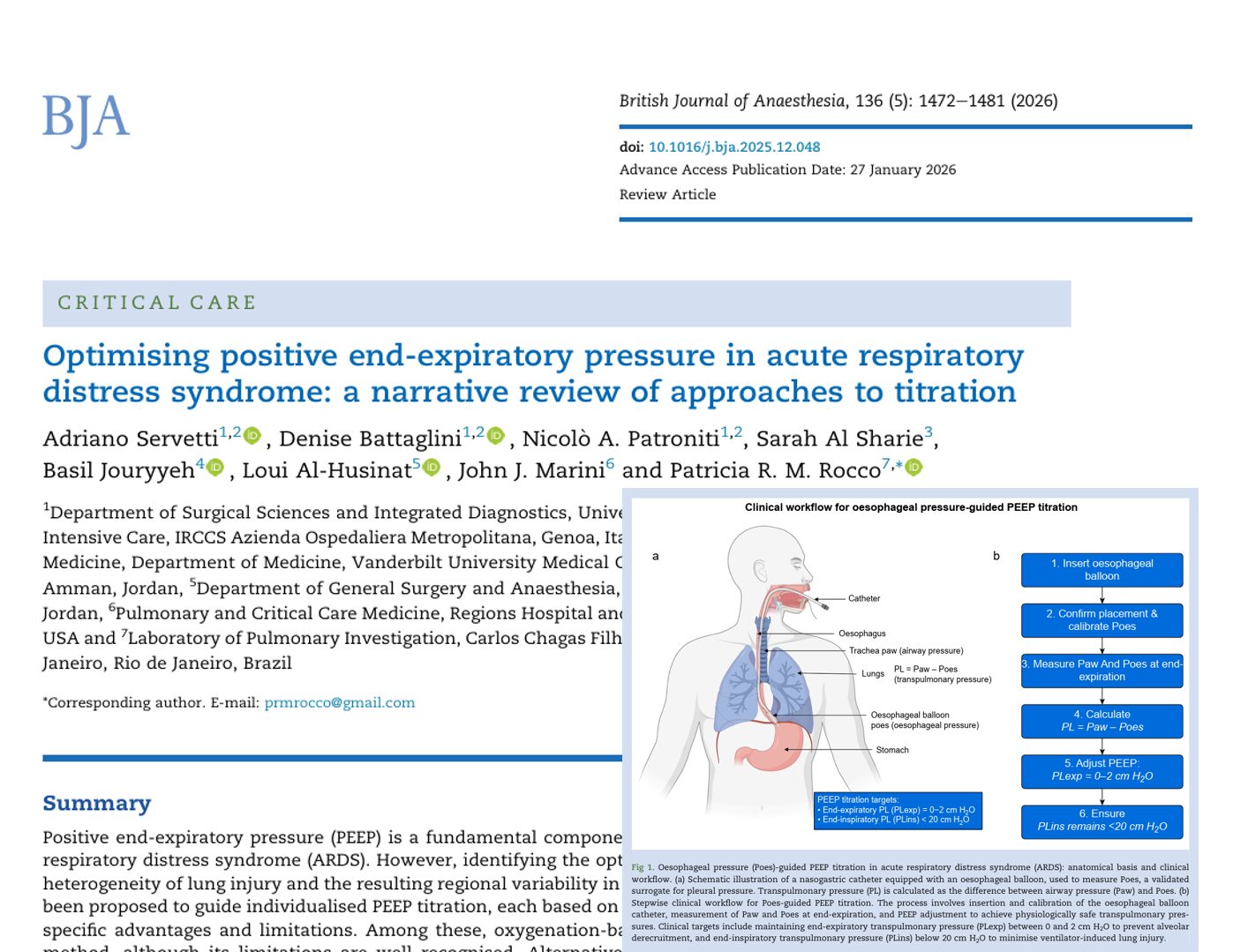





Acute respiratory distress syndrome (ARDS) remains one of the most challenging conditions managed in intensive care medicine. Mechanical ventilation is lifesaving, yet it can also worsen lung injury if not carefully adjusted. Among all ventilator settings, positive end-expiratory pressure (PEEP) is one of the most critical and controversial.
A 2026 narrative review published in the British Journal of Anaesthesia examined modern approaches to PEEP titration in ARDS and highlighted the growing shift toward personalized ventilation strategies.
What is PEEP?
Positive end-expiratory pressure refers to the pressure maintained in the lungs at the end of expiration during mechanical ventilation.
Its goals include:
- Preventing alveolar collapse
- Improving oxygenation
- Increasing functional residual capacity
- Reducing the cyclic opening and closing of alveoli
- Minimizing ventilator-induced lung injury (VILI)
In ARDS, many alveoli become fluid-filled or collapsed. PEEP helps keep recruitable alveoli open and improves gas exchange.
However, excessive PEEP can overdistend already open lung regions and impair hemodynamics.
The challenge is identifying the “optimal” PEEP for each individual patient.
Why PEEP optimization is difficult in ARDS
ARDS lungs are highly heterogeneous.
Some lung regions are:
- Fully aerated
- Poorly aerated
- Collapsed
- Consolidated
This concept is often described as the “baby lung,” meaning that only a small portion of the lung remains available for ventilation.
Because recruitability differs among patients, a fixed PEEP strategy may cause:
- Under-recruitment in some patients
- Overdistension in others
The review emphasizes that personalized PEEP titration is essential rather than relying on universal PEEP tables.
Traditional oxygenation-based PEEP titration
Historically, clinicians adjusted PEEP according to oxygenation response, particularly the PaO2/FIO2 ratio.
How it works
PEEP is increased stepwise while monitoring:
- Arterial oxygenation
- Oxygen saturation
- PaO2/FIO2 ratio
Improved oxygenation was traditionally interpreted as successful alveolar recruitment.
Limitations of oxygenation-guided PEEP
The review highlights several major limitations:
Improved oxygenation does not always mean safer ventilation
A patient may show better oxygenation despite:
- Regional overdistension
- Increased lung stress
- Ventilation-perfusion mismatch
Hemodynamic changes influence oxygenation
PEEP affects:
- Cardiac output
- Pulmonary blood flow
- Intrapulmonary shunt
As a result, changes in oxygenation may not accurately reflect alveolar recruitment.
Fixed PEEP/FIO2 tables ignore patient variability
Different patients have different:
- Lung recruitability
- Chest wall mechanics
- Disease distribution
This makes standardized protocols imperfect.
Compliance-based and driving pressure-guided titration
Modern strategies increasingly focus on respiratory mechanics rather than oxygenation alone.
What is driving pressure?
Driving pressure (ΔP) is calculated as:
ΔP=Pplat−PEEP
Where:
- Pplat = plateau pressure
- PEEP = positive end-expiratory pressure
Driving pressure reflects the cyclic stress applied to the functional “baby lung.”
Why driving pressure matters
Studies cited in the review demonstrate that higher driving pressure is strongly associated with increased mortality in ARDS.
Reducing driving pressure may:
- Lower mechanical stress
- Reduce overdistension
- Minimize cyclic alveolar collapse
- Improve survival
Compliance-guided PEEP titration
Respiratory system compliance is calculated as:
Crs=VT/ΔP
Where:
- Crs = respiratory system compliance
- VT = tidal volume
- ΔP = driving pressure
Principle
As recruitable alveoli reopen:
- Compliance improves
- Driving pressure decreases
Once overdistension occurs:
- Compliance worsens
- Driving pressure rises
The “optimal” PEEP is therefore the level associated with:
- Highest compliance
- Lowest driving pressure
Advantages of mechanics-guided PEEP
Benefits include:
- Better individualisation
- Reduced physiological dead space
- Lower risk of VILI
- Improved lung protection
However, these methods still have limitations because they assess global rather than regional lung behaviour.
Recruitment-to-inflation ratio
The review describes the recruitment-to-inflation (R/I) ratio as a practical bedside tool for assessing recruitability.
How it works
PEEP is reduced abruptly, typically from:
- 15 cm H2O
to - 5 cm H2O
The clinician measures:
- Changes in end-expiratory lung volume
- Changes in driving pressure
Interpretation
Low R/I ratio
Suggests:
- Poor recruitability
- Higher risk of overdistension with increased PEEP
High R/I ratio
Suggests:
- Greater recruitability
- Potential benefit from higher PEEP
This technique uses only standard ventilator data and does not require advanced imaging.
Oesophageal pressure-guided PEEP titration
One of the most physiologically advanced approaches involves oesophageal pressure monitoring.
Why oesophageal pressure matters
Airway pressure alone cannot distinguish:
- Lung pressure
from - Chest wall pressure
Oesophageal pressure acts as a surrogate for pleural pressure.
This allows calculation of transpulmonary pressure:
PL=Paw−Poes
Where:
- PL = transpulmonary pressure
- Paw = airway pressure
- Poes= oesophageal pressure
Clinical targets
The review recommends:
End-expiratory transpulmonary pressure
Target:
- 0–2 cm H2O
End-inspiratory transpulmonary pressure
Target:
- Less than 20 cm H2O
These targets aim to:
- Prevent alveolar collapse
- Avoid overdistension
Patients who may benefit most
This approach is particularly useful in:
- Obesity
- Increased intra-abdominal pressure
- Chest wall edema
- Altered thoracoabdominal mechanics
In such patients, plateau pressure alone may underestimate true lung stress.
Imaging-guided PEEP titration
Modern imaging techniques are increasingly used to personalize ventilation.
The review discusses several modalities.
Chest CT: the gold standard
Computed tomography remains the reference standard for assessing recruitability.
Advantages
Chest CT provides:
- High-resolution anatomical imaging
- Quantification of recruitable lung
- Identification of focal vs non-focal ARDS
Patients with non-focal ARDS often demonstrate:
- Greater recruitability
- Better response to higher PEEP
Limitations
Despite its accuracy, CT has drawbacks:
- Radiation exposure
- Need for patient transport
- Limited bedside availability
- Resource intensity
For this reason, CT is often reserved for selected patients or research settings.
Electrical impedance tomography (EIT)
Electrical impedance tomography is gaining popularity as a bedside monitoring tool.
How EIT works
Electrodes placed around the thorax measure impedance changes during ventilation.
This provides:
- Real-time regional ventilation maps
- Breath-by-breath assessment
- Dynamic monitoring of recruitment and overdistension
Benefits of EIT-guided PEEP
The review reports that EIT-guided titration may improve:
- Oxygenation
- Compliance
- Driving pressure
- Ventilation homogeneity
Several studies demonstrated reductions in:
- Mechanical power
- Regional overdistension
Limitations
Challenges include:
- Limited spatial resolution
- Need for expertise
- Reduced accuracy in obesity or edema
- Lack of universal interpretation standards
Even so, EIT is increasingly viewed as one of the most promising bedside tools for personalized ventilation.
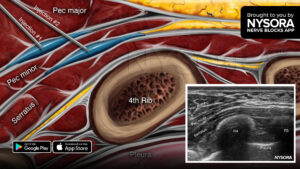
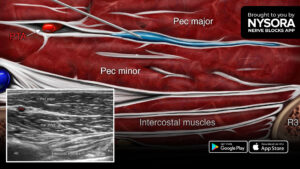
Lung ultrasound (LUS)
Lung ultrasound has become widely used in critical care.
Advantages of lung ultrasound
LUS is:
- Portable
- Radiation-free
- Repeatable
- Bedside accessible
It can identify:
- B-lines
- Consolidation
- Pleural effusions
- Recruitment patterns
Lung ultrasound scoring
Several scoring systems evaluate regional aeration changes during PEEP adjustments.
Recruitment may appear as:
- Reduction in B-lines
- Re-aeration of consolidated regions
The review notes a good correlation between lung ultrasound findings and CT-based aeration assessment.
Integrated multimodal PEEP strategies
The review strongly supports combining:
- Respiratory mechanics
- Physiological monitoring
- Imaging techniques
Rather than relying on a single variable.
Key clinical insights from the review
Important takeaways include:
- Better oxygenation does not always mean safer ventilation
- Driving pressure is a powerful predictor of mortality
- Transpulmonary pressure monitoring improves precision
- EIT and lung ultrasound enable bedside regional assessment
- Personalized PEEP is superior to fixed protocols
Conclusion
PEEP optimization remains one of the most important yet complex aspects of ARDS management.
Traditional oxygenation-guided methods are simple but insufficient for true lung-protective ventilation. Modern approaches increasingly emphasize:
- Driving pressure minimization
- Compliance optimisation
- Transpulmonary pressure assessment
- Regional imaging
The future of ARDS ventilation lies in integrated, physiology-based personalized strategies that balance recruitment with protection against overdistension.
As bedside imaging and monitoring technologies continue to evolve, clinicians may achieve increasingly precise and safer ventilatory support for critically ill patients with ARDS.
Reference: Servetti A et al. Optimising positive end-expiratory pressure in acute respiratory distress syndrome: a narrative review of approaches to titration. Br J Anaesth. 2026;136:1472-1481.
Download the Anesthesia Assistant App HERE for step-by-step guidance, case support, troubleshooting, and educational insights at the point of care.