Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About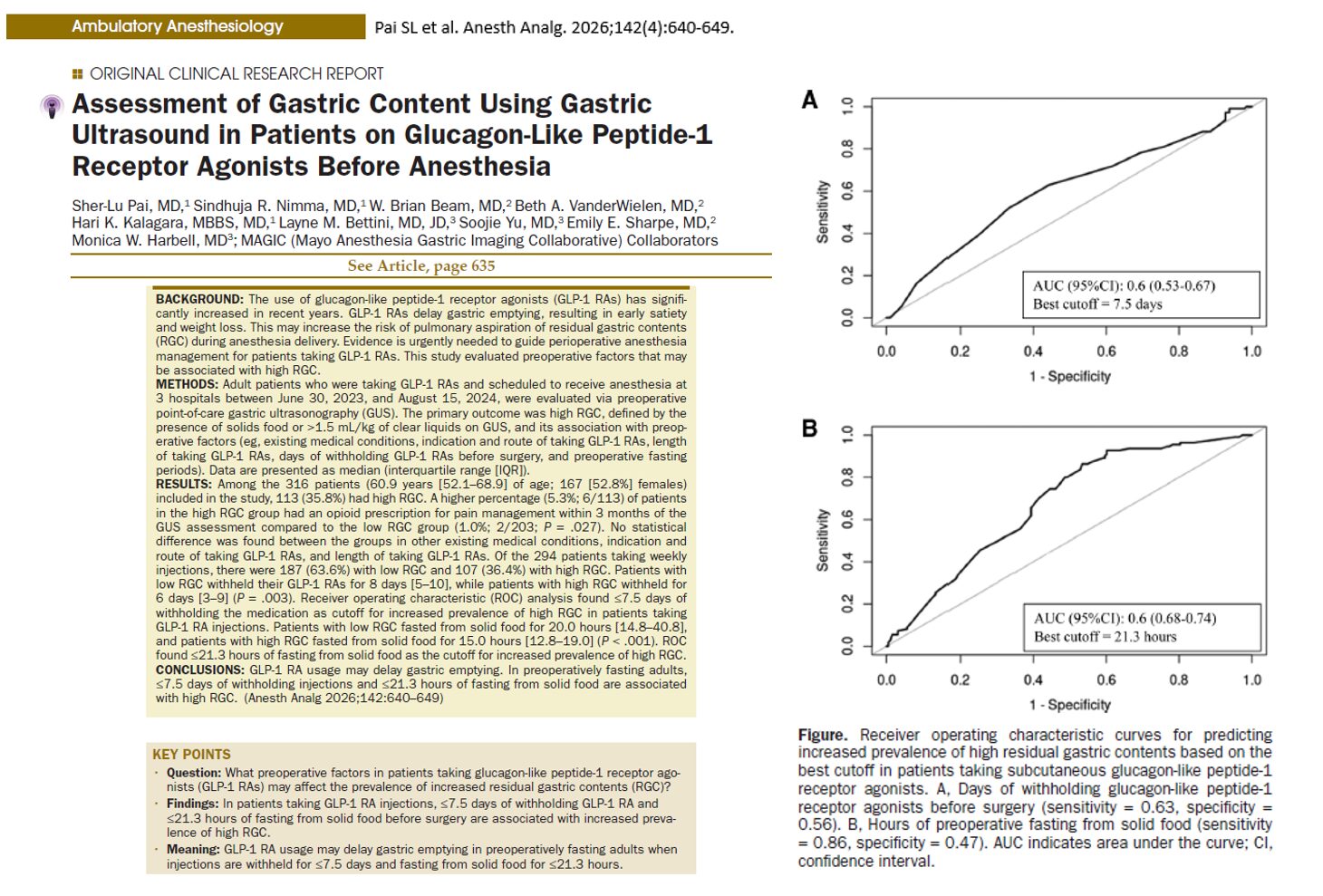





Introduction
The widespread adoption of glucagon-like peptide-1 receptor agonists (GLP-1 RAs), such as semaglutide and tirzepatide, has transformed the management of type 2 diabetes mellitus and obesity. However, emerging evidence is raising important concerns for anesthesiologists and perioperative clinicians.
A new clinical study from the Mayo Clinic, published in Anesthesia & Analgesia (2026), provides critical insights into how these medications influence gastric physiology and potentially increase the risk of pulmonary aspiration during anesthesia.
What are GLP-1 receptor agonists?
GLP-1 receptor agonists are incretin-based therapies that:
- Enhance glucose-dependent insulin secretion
- Suppress glucagon release
- Slow gastric emptying
- Promote satiety and weight loss
Common medications include:
- Semaglutide
- Tirzepatide
- Dulaglutide
- Liraglutide
Their ability to delay gastric emptying is central to both their therapeutic benefits and perioperative risks.
Why delayed gastric emptying matters in anesthesia
Pulmonary aspiration occurs when gastric contents enter the lungs during anesthesia, potentially leading to:
- Aspiration pneumonitis
- Acute respiratory distress syndrome (ARDS)
- Increased perioperative morbidity and mortality
Standard fasting guidelines (e.g., 6–8 hours for solids) aim to minimize this risk. However, GLP-1 RAs may disrupt this safety margin.
Study overview
Design and population
- 316 adult patients on GLP-1 RAs
- Conducted across three Mayo Clinic centers
- Preoperative evaluation using gastric ultrasound (GUS)
Definition of high-risk gastric content
- Solid food present
- Or >1.5 mL/kg of gastric fluid volume
Key findings
-
High prevalence of residual gastric contents
- 35.8% of patients had high residual gastric content (RGC)
- This occurred despite adherence to fasting guidelines
-
Insufficient medication withholding increases risk
- Patients with high RGC withheld GLP-1 RAs for a shorter duration
- Critical cutoff: ≤7.5 days before surgery increased risk
-
Fasting duration is crucial
- Patients with high RGC fasted for shorter periods
- Critical cutoff: ≤21.3 hours for solid food
This is significantly longer than standard fasting recommendations.
-
Opioid use may worsen gastric retention
- Higher prevalence of recent opioid use in the high RGC group
- Suggests an additive effect on gastric motility
-
No difference in indication or duration of therapy
- Whether patients used GLP-1 RAs for diabetes or weight loss did not affect risk
- Duration of therapy was not a significant predictor
Interpretation
- Withholding ≤7.5 days → higher risk of retained gastric contents
- Fasting ≤21.3 hours → strongest predictor of high RGC
These thresholds optimize sensitivity and specificity for detecting risk.
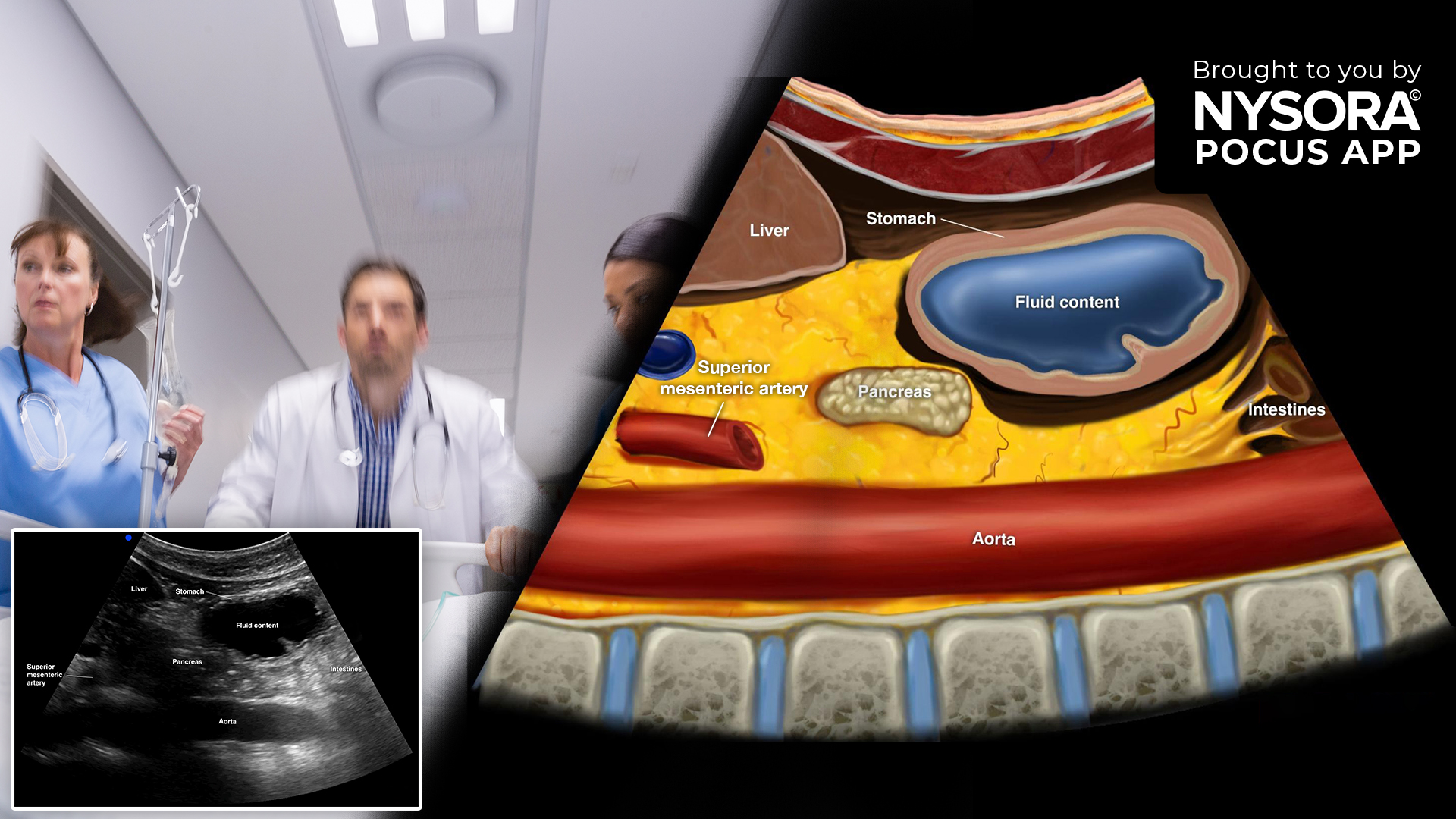
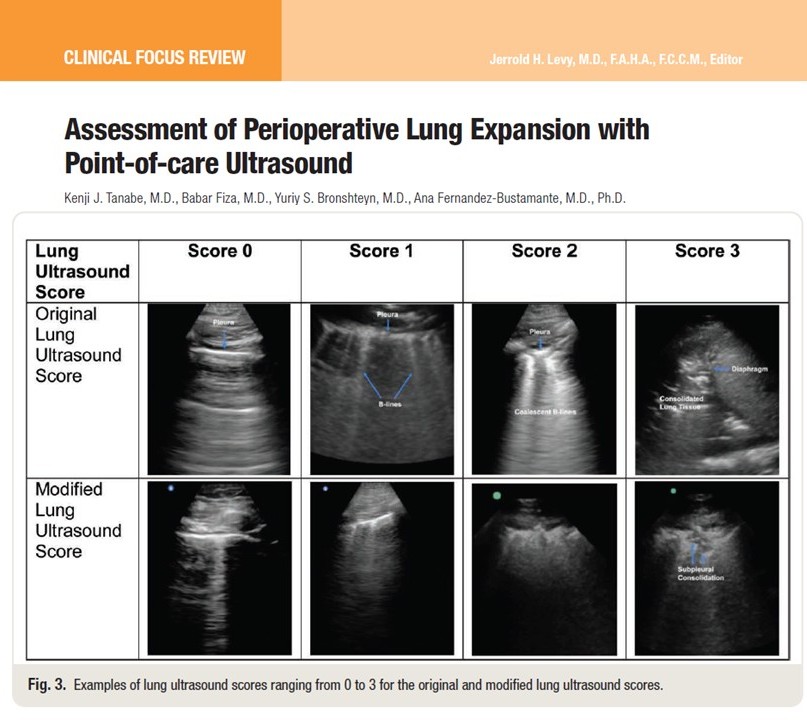
How gastric ultrasound helps
What is gastric ultrasound (GUS)?
A point-of-care imaging technique used preoperatively to assess:
- Gastric volume
- Nature of contents (empty, liquid, or solid)
Clinical advantages
- Non-invasive
- Rapid bedside assessment
- Guides anesthesia decision-making
Impact in the study
- 38.9% of patients had changes in anesthesia management
- High-risk patients often received:
- Rapid sequence induction (RSI)
- Procedure delay or cancellation in some cases
Clinical implications
-
Standard fasting guidelines may be inadequate
GLP-1 RA users may still have significant gastric contents despite:
- 8 hours fasting
- Adherence to guidelines
-
Individualized risk assessment is essential
Clinicians should consider:
- Duration of drug withholding
- Fasting duration
- Presence of GI symptoms
- Use of opioids or other motility-altering drugs
-
Anesthesia plans may need modification
For high-risk patients:
- Rapid sequence induction
- Airway protection strategies
- Consider delaying elective procedures
Step-by-step perioperative management approach
-
Preoperative assessment
- Review GLP-1 RA use:
- Type
- Dose
- Last administration
- Evaluate symptoms:
- Nausea
- Vomiting
- Bloating
-
Medication management
- Consider withholding:
- Daily dosing → at least 24 hours
- Weekly dosing → up to 7 days or more
-
Fasting optimization
- Extend fasting duration for solids:
- Aim for >21 hours if feasible
- Use clear liquids as per guidelines
-
Perform gastric ultrasound (if available)
- Identify high-risk patients
- Quantify gastric volume
-
Adjust anesthesia plan
- Low risk:
- Standard induction
- High risk:
- Rapid sequence induction
- Airway protection
- Possible delay
Evolving clinical guidelines
Current recommendations vary:
- ASA (2023):
- Hold weekly GLP-1 RAs for 7 days
- Updated guidance (2024):
- Continue in low-risk patients
- Consider a liquid diet for 24 hours
- UK consensus (2025):
- Use gastric ultrasound for risk stratification
Limitations of the study
- Retrospective design
- Limited sample size (316 patients)
- Selection bias (patients more likely to receive ultrasound)
- Limited data on oral GLP-1 formulations
Future directions
Further research is urgently needed to:
- Define optimal fasting durations
- Establish standardized perioperative protocols
- Evaluate real-world aspiration risk
Conclusion
The rise of GLP-1 receptor agonists presents a new challenge in perioperative medicine. This study highlights that:
- Delayed gastric emptying is clinically significant
- Standard fasting guidelines may be insufficient
- Gastric ultrasound is a valuable tool for risk stratification
As GLP-1 use continues to expand, anesthesiologists must adapt their practices to ensure patient safety.
For more information, refer to the full article in Anesthesia & Analgesia
Pai SL, Nimma SR, Beam WB, et al. Assessment of Gastric Content Using Gastric Ultrasound in Patients on Glucagon-Like Peptide-1 Receptor Agonists Before Anesthesia. Anesth Analg. 2026;142(4):640-649.
Download the POCUS App HERE for step-by-step guidance on gastric ultrasound and more!