Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About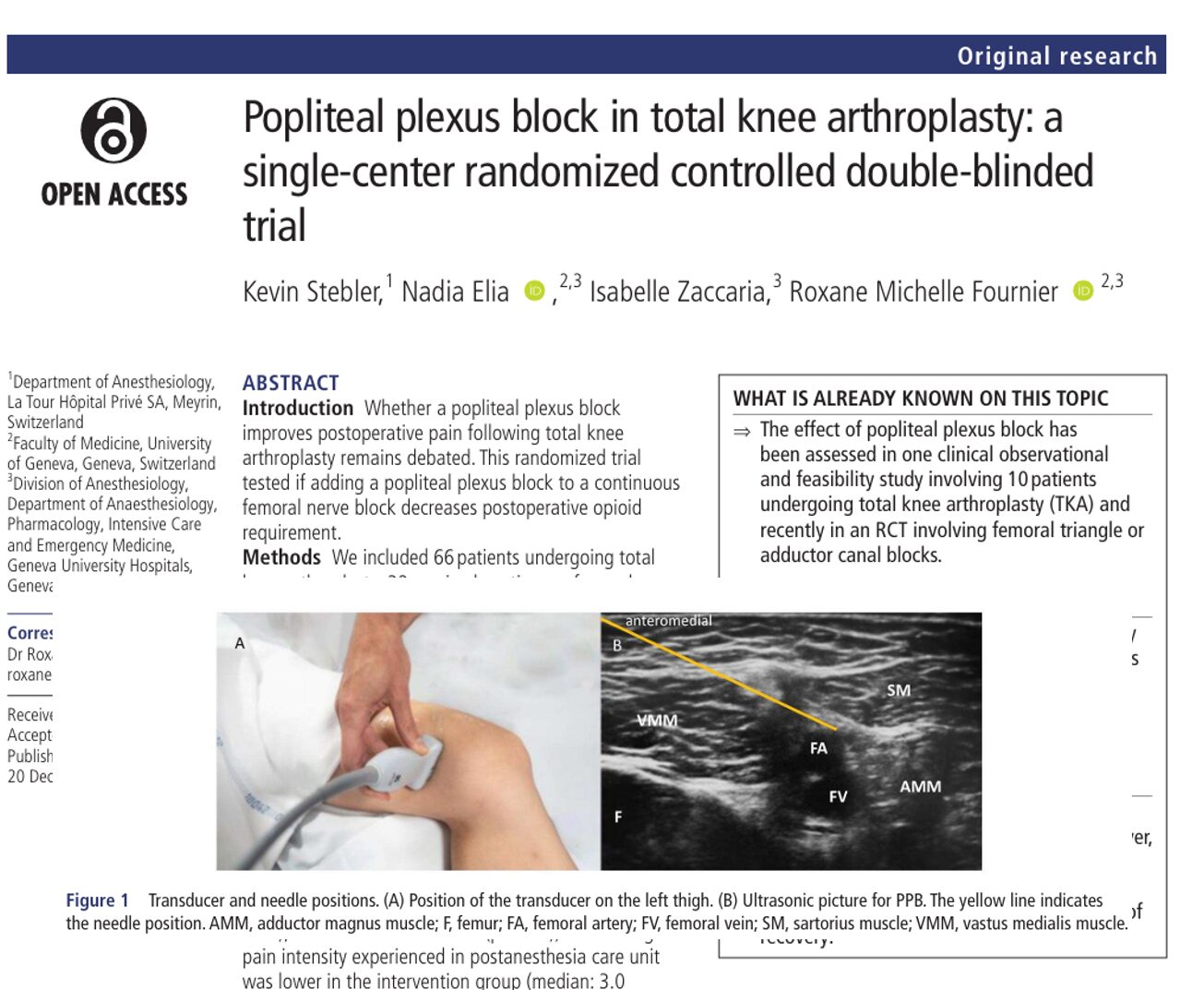





Introduction
Total knee arthroplasty (TKA) remains one of the most commonly performed orthopedic procedures worldwide, yet postoperative pain continues to be a major barrier to early mobilization, patient satisfaction, and the implementation of enhanced recovery protocols. While multimodal analgesia strategies have advanced significantly, achieving effective control of posterior knee pain without compromising motor function remains a persistent challenge. Traditional approaches such as femoral nerve blocks (FNB) or adductor canal blocks (ACB) primarily address anterior knee pain, leaving a substantial proportion of patients—67–89%—with residual posterior discomfort.
In response, newer motor-sparing regional techniques have gained attention, including the IPACK block, genicular nerve blocks, and selective tibial nerve blocks. Among these, the popliteal plexus block (PPB) has emerged as a promising alternative, aiming to selectively target posterior knee innervation while preserving motor function. However, robust clinical evidence supporting its routine use remains limited.
The randomized, double-blind trial by Stebler et al. provides timely insight into this evolving field by evaluating whether adding a PPB to a continuous femoral nerve block (CFNB) meaningfully reduces opioid consumption and improves pain outcomes following TKA. This study is particularly relevant for clinicians seeking incremental improvements in analgesia while balancing safety, efficiency, and functional recovery in modern perioperative care pathways.
Study objective and methods
Objective
To determine whether adding a popliteal plexus block (PPB) to a continuous femoral nerve block (CFNB) reduces postoperative opioid consumption in patients undergoing TKA.
Study design
- Single-center, randomized, double-blind controlled trial
- Registered and CONSORT-compliant
Participants
- Total: 66 patients
- Groups: CFNB + PPB (n=32) and CFNB alone (n=34)
- ASA I–III patients undergoing elective TKA
Intervention
All patients received:
- General anesthesia
- Continuous femoral nerve catheter
- Standard multimodal analgesia (paracetamol, NSAIDs, opioids PRN)
Intervention group received:
- Ultrasound-guided PPB with 15 mL ropivacaine 0.5%
Primary outcome
- 12-hour cumulative morphine-equivalent consumption
Secondary outcomes
- Pain scores (VAS 0–10) at multiple timepoints
- Opioid consumption at PACU, 24h, 48h
- Pain location (posterior vs anterior knee)
- Motor strength (to assess motor-sparing effect)
- Adverse events
Statistical approach
- Intention-to-treat primary analysis
- Wilcoxon tests for comparisons
- Power calculation based on detecting a 5 mg opioid reduction
Key findings
The results highlight a statistically significant but clinically modest benefit of adding PPB:
Primary outcome
12-hour opioid consumption:
- PPB group: 6.1 mg (IQR 0.5–14.5)
- Control: 10 mg (IQR 5–17.3)
- p = 0.04
This represents a reduction of ~4 mg morphine equivalent.
Secondary outcomes
PACU pain scores (mean):
- Lower in PPB group: 2 vs 3
- p = 0.01
Posterior knee pain (PACU):
- PPB: 34.4%
- Control: 61.8%
- p = 0.03
Intraoperative opioid use (sufentanil):
- Lower in the PPB group
- p = 0.02
24–48 hour outcomes:
- No significant differences in opioid use or pain scores
Safety
- No evidence of sciatic nerve injury
- No motor weakness differences between groups
- Transient neurologic events occurred only in the control group
Procedure efficiency
- Median PPB time: 5 minutes
Differences in opioid consumption and pain scores diminish after 24 hours, emphasizing the short-lived benefit.
Clinical implications
This study reinforces that PPB can:
- Provide early posterior knee analgesia
- Reduce immediate postoperative opioid requirements
- Maintain motor-sparing properties, supporting early mobilization
However, the magnitude of benefit is small, raising questions about whether the additional procedure justifies routine implementation—especially in already optimized multimodal pathways.
Clinical pearls
- PPB targets the popliteal plexus and posterior obturator contributions, addressing a known analgesic gap.
- It is quick (~5 min) and technically feasible under ultrasound.
- Unlike sciatic nerve blocks, PPB preserves motor function, reducing fall risk.
- Best viewed as an adjunct, not a replacement, in multimodal analgesia.
- Benefits are front-loaded (within the first 12–24 hours)—plan accordingly.
Future research
The authors highlight several important next steps:
Direct comparisons with:
- IPACK block
- Local infiltration analgesia (LIA)
Evaluation of:
- Optimal local anesthetic volume and concentration
- Duration of analgesia
Shift toward patient-centered outcomes:
- Quality of recovery
- Functional mobility
- Satisfaction
Additionally, the study demonstrates feasibility for larger trials despite pandemic-related recruitment challenges.
Conclusion
The addition of a popliteal plexus block to a continuous femoral nerve block in TKA results in a statistically significant reduction in early opioid consumption and improved immediate postoperative pain control. However, the clinical impact is modest and short-lived, with benefits dissipating after 24 hours.
While PPB is a safe, efficient, and motor-sparing technique, its routine use should be weighed against its incremental benefit. It may be most valuable in select patients or enhanced recovery protocols where even small opioid reductions matter.
Practical tip
If you’re already using CFNB or ACB for TKA, consider adding PPB selectively—not routinely.
Use it in:
- Patients with high opioid sensitivity or risk
- Cases where posterior knee pain is anticipated to be significant
- Settings aiming for ultra-fast recovery protocols
But remember: A 4 mg morphine reduction is helpful—but not practice-changing on its own.
For more information, refer to the full article in RAPM.
Stebler K, Elia N, Zaccaria I, Fournier RM. Popliteal plexus block in total knee arthroplasty: a single-center randomized controlled double-blinded trial. Reg Anesth Pain Med. 2026 Mar 5;51(3):309-316.
Stay ahead in regional anesthesia—subscribe to the NYSORA Nerve Blocks App for 70+ blocks and expert insights.