
- Learn
-
Apps
View all apps
Veterinary
 VetRA App
VetRA App

- Books
- Events
- News
- Partners
- About
- For Clinicians
 VetRA App
VetRA App
This manual is the most up-to-date resource on best clinical practices and practical case management in anesthesiology. It is an essential guide for students, residents, and experienced practitioners to confidently manage complex clinical scenarios.


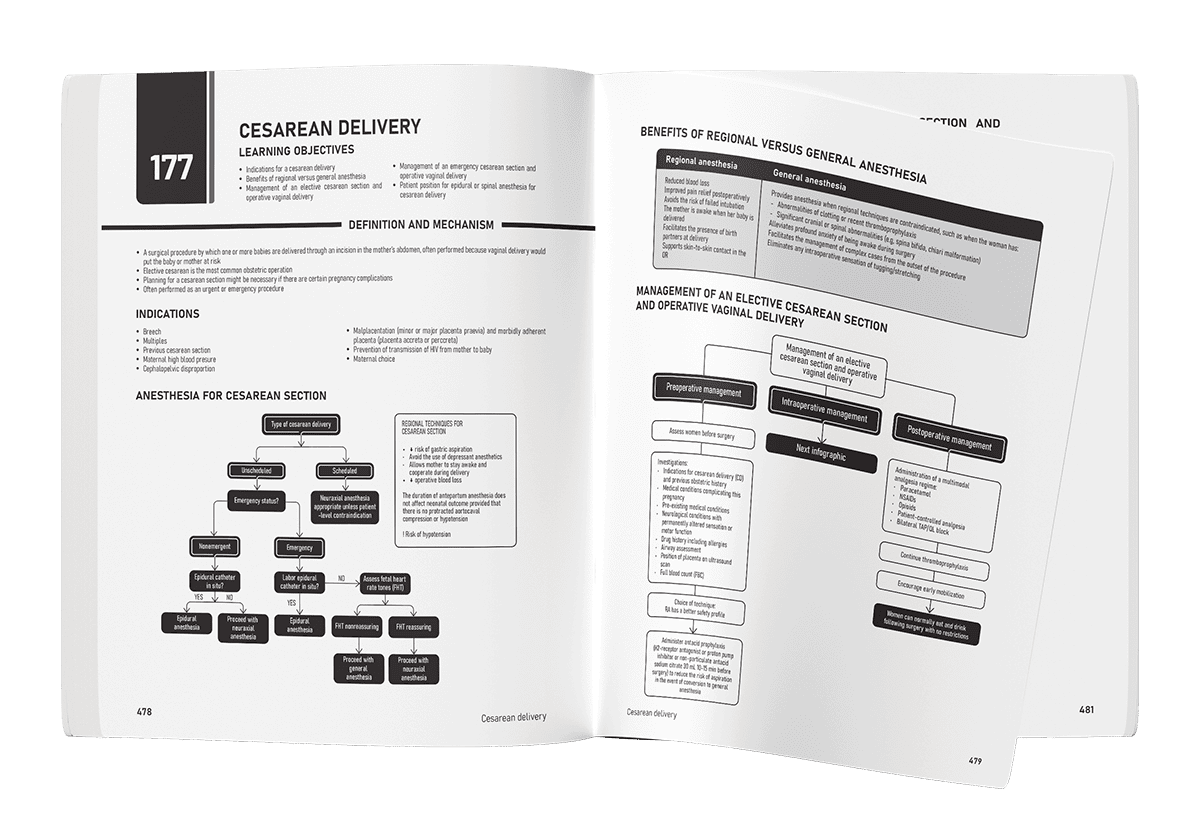

Elective cesarean section remains one of the most frequently performed surgical procedures worldwide. Although it is a routine operation, postoperative pain can be substantial and may significantly affect maternal recovery, infant care, breastfeeding success, mobilisation, sleep quality and overall wellbeing. Poorly controlled postoperative pain has also been linked to an increased risk of chronic postsurgical pain and postpartum depression. In 2026, the PROcedure SPEcific Postoperative Pain ManagemenT (PROSPECT) Working Group published an updated systematic review and evidence-based guideline for pain management after elective cesarean section performed under neuraxial anesthesia. The review evaluated 61 randomized controlled trials and numerous systematic reviews and meta-analyses to determine the safest and most effective analgesic strategies. Why effective pain management matters Post-cesarean pain is more than a comfort issue. Effective analgesia is essential for: Early maternal mobilisation Improved respiratory function Enhanced mother-infant bonding Successful breastfeeding Reduced opioid consumption Faster recovery Improved patient satisfaction Reduced risk of chronic pain development Lower likelihood of postpartum depression Researchers highlighted that uncontrolled pain can negatively affect both patient-centred and healthcare-centred outcomes, making evidence-based pain management a critical component of obstetric care. Key recommendations at a glance The updated PROSPECT guideline recommends a multimodal analgesic strategy. Core recommendations Administer paracetamol unless contraindicated. Administer a non-steroidal anti-inflammatory drug (NSAID) unless contraindicated. Give intravenous dexamethasone 8–10 mg after delivery. Use intrathecal morphine 50–100 micrograms or intrathecal diamorphine 300 micrograms. Continue regular paracetamol and NSAIDs postoperatively. Reserve opioids primarily as rescue medication. Consider regional analgesia techniques if neuraxial opioids are not used. Use surgical approaches associated with lower postoperative pain. The role of neuraxial opioids Intrathecal morphine remains the gold standard The guideline strongly supports intrathecal morphine at doses between 50 and 100 micrograms. Investigators found that higher doses did not significantly improve pain control but increased adverse effects such as: Pruritus Nausea […]
Postpartum headache is one of the most common neurologic complaints after childbirth. Nearly 40% of postpartum patients develop headaches in the early puerperium. While many are benign primary headaches, such as migraine or tension-type headache, a substantial proportion are secondary headaches caused by potentially life-threatening conditions. A new review published in Current Opinion in Anesthesiology highlights the importance of recognizing uncommon but dangerous postpartum headache syndromes that may mimic postdural puncture headache (PDPH) or preeclampsia. These rare conditions include: Cerebral venous sinus thrombosis (CVST) Posterior reversible encephalopathy syndrome (PRES) Reversible cerebral vasoconstrictive syndrome (RCVS) Pituitary apoplexy Subdural hematoma Subarachnoid hemorrhage Intracranial tumors Lymphocytic hypophysitis The review emphasizes that delayed diagnosis remains common because postpartum fatigue, hormonal fluctuations, sleep deprivation, and stress can obscure warning signs. Cerebral venous sinus thrombosis (CVST) What is CVST? CVST is a form of stroke caused by thrombosis within the cerebral venous sinuses. The obstruction impairs venous drainage from the brain, increasing intracranial venous pressure. Pregnancy and the puerperium significantly increase risk because of the prothrombotic state associated with childbirth. Approximately 20% of CVST cases occur during pregnancy or postpartum. Symptoms Patients may develop: Severe headache Focal neurologic deficits Seizures Altered mental status Visual symptoms An important distinguishing feature is positional behavior opposite to PDPH: CVST headache often worsens while supine PDPH typically worsens upright Diagnosis Preferred imaging includes: Magnetic resonance venography (MRV) CT venography in selected cases Treatment Management usually involves: Systemic anticoagulation Neurologic monitoring Occasionally, thrombectomy or thrombolysis Early recognition substantially improves outcomes. Posterior reversible encephalopathy syndrome (PRES) Understanding PRES PRES is characterized by vasogenic cerebral edema, particularly affecting posterior brain regions. The condition is strongly linked to: Severe hypertension Preeclampsia Eclampsia HELLP syndrome Studies suggest nearly all patients with eclamptic seizures demonstrate radiographic evidence of PRES. Clinical features Common manifestations include: Headache Visual […]
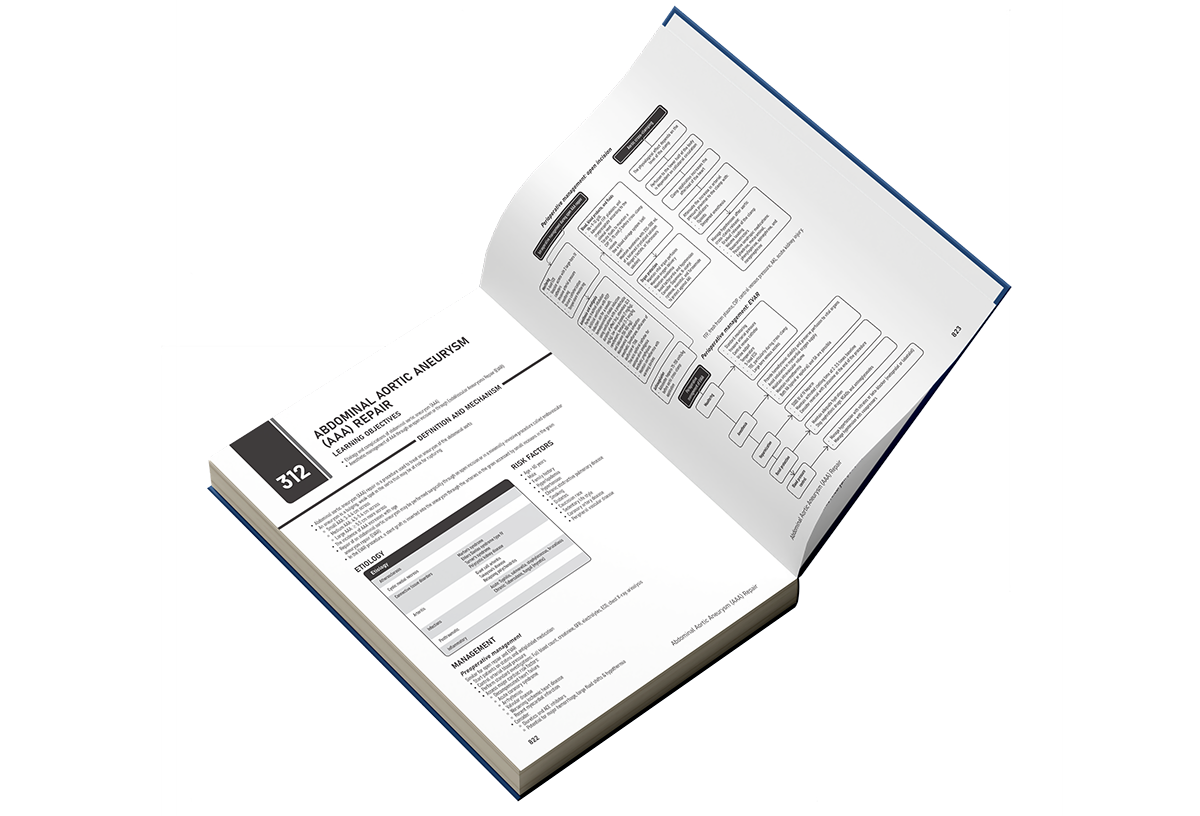
The Anesthesiology Manual is offers over 300 topics to guide clinicians through perioperative anesthetic management of diverse patients.
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About