Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About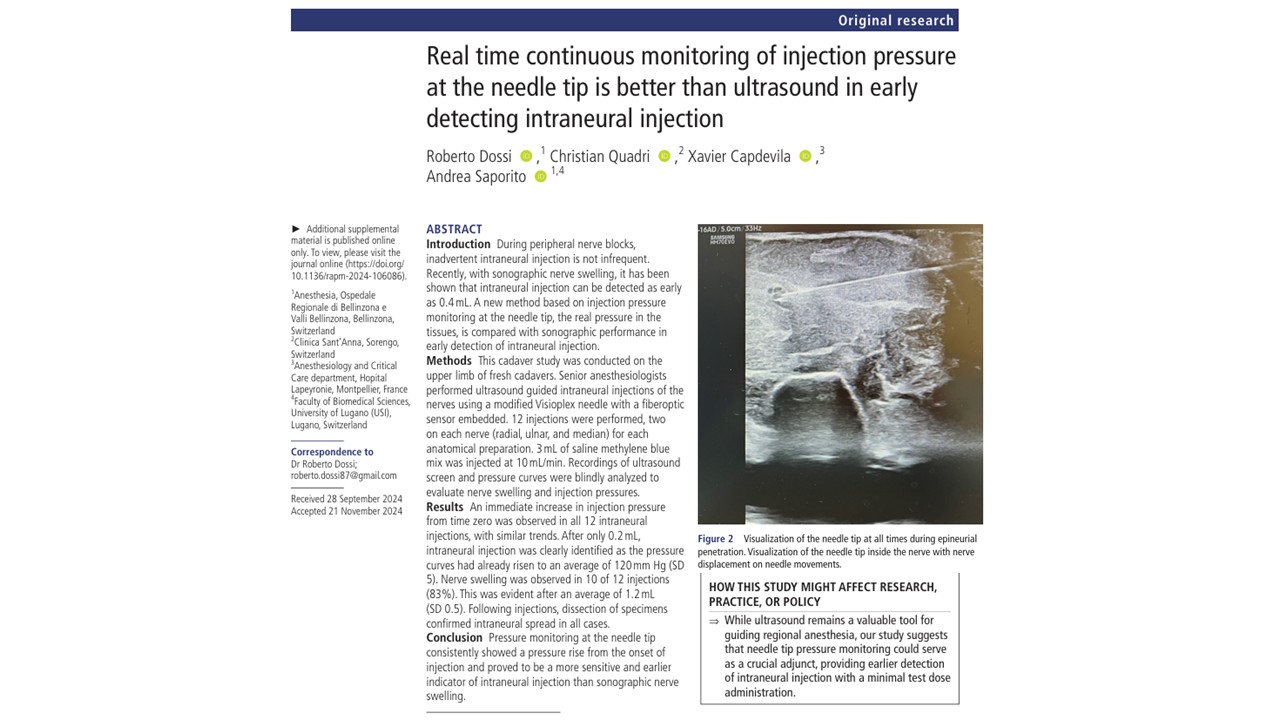
Introduction
Intraneural injection remains one of the most feared complications in regional anesthesia. Despite widespread adoption of ultrasound guidance, unintentional intraneural injection still occurs—even in experienced hands. Ultrasound has improved needle visualization and procedural accuracy, but the earliest sonographic signs of intraneural injection may still appear only after potentially harmful pressure has already developed within the nerve.
A new cadaveric study by Dossi et al. evaluated whether real-time continuous pressure monitoring directly at the needle tip could identify intraneural injection earlier than ultrasound-based nerve swelling. Their findings suggest that needle-tip pressure monitoring may detect intraneural injection almost immediately, well before visible nerve swelling appears on ultrasound.
This study adds important insight to the evolving discussion surrounding injection pressure monitoring, nerve injury prevention, and multimodal safety strategies during peripheral nerve blocks.
Why Intraneural Injection Still Matters
Regional anesthesia has transformed perioperative care by improving postoperative analgesia, reducing opioid requirements, and facilitating enhanced recovery pathways. However, peripheral nerve blocks are not without risk. Neurologic complications remain uncommon but potentially devastating, ranging from transient paresthesia to persistent nerve dysfunction.
Even with ultrasound guidance, inadvertent intraneural injection continues to occur. Previous literature has estimated rates of unintended intraneural injection around 16–17%, while postoperative neurologic symptoms after peripheral nerve blocks may occur in up to 2.6–16% of patients, depending on definitions and follow-up methods.
Ultrasound guidance offers clear advantages, but it also has limitations:
- Needle visualization can be imperfect
- Image quality varies between patients
- Deep blocks and obesity reduce resolution
- Operator experience strongly affects interpretation
- Sonographic nerve swelling may appear relatively late
Importantly, nerve swelling is currently considered the only direct sonographic sign of intraneural injection. By the time swelling becomes visible, pressure within the low-compliance intraneural compartment may already have reached potentially harmful levels.
This raises a crucial question:
Can another monitoring strategy identify intraneural injection earlier than ultrasound alone?
Study Objective
The authors aimed to determine whether real-time continuous monitoring of injection pressure directly at the needle tip could detect intraneural injection earlier than ultrasound-based visualization of nerve swelling.
The investigators also sought to identify:
- The minimum injected volume associated with the pressure rise
- A possible new pressure threshold for early warning
- Whether needle-tip pressure monitoring could improve safety during regional anesthesia
Study Design and Methods
This was a cadaveric study performed on upper extremity nerves in fresh cadavers at the ICLO Teaching and Research Center in Verona, Italy.
The investigators targeted:
- Median nerve
- Radial nerve
- Ulnar nerve
Two injections were performed in each nerve on each cadaver preparation, resulting in a total of 12 intraneural injections.
Technique
Experienced anesthesiologists performed ultrasound-guided intraneural injections using a modified Visioplex needle equipped with an embedded fiberoptic pressure sensor. The system continuously measured pressure directly at the needle tip in real time.
Unlike conventional in-line pressure monitors, this technology measured the “true” tissue pressure at the needle tip itself rather than pressure transmitted through tubing and syringes. The sensor had:
- Resolution: 0.1 mm Hg
- Accuracy: ±10 mm Hg
Pressure curves were displayed in real time on a tablet interface and recorded throughout the injection.
Intraneural Needle Placement Criteria
The authors used strict sonographic criteria to confirm intraneural needle tip position:
- Continuous visualization of the needle tip
- Indentation followed by puncture of the epineurium
- Visualization of the needle tip within the nerve
- Nerve displacement during needle movement
Injection Protocol
After confirming intraneural positioning:
- 3 mL saline/methylene blue solution was injected
- Injection speed was standardized at 10 mL/min using a syringe pump
The investigators simultaneously recorded:
- Ultrasound images
- Pressure monitoring curves
Later, blinded reviewers independently analyzed ultrasound recordings to determine the earliest visible nerve swelling and the corresponding injected volume. After injections, cadaver dissections confirmed intraneural spread in all cases.
Key Findings
- Pressure Increased Immediately in Every Intraneural Injection
The most striking finding was the consistency of pressure rise.
All 12 intraneural injections demonstrated an immediate increase in pressure from the onset of injection, with remarkably similar curve profiles across nerves.
This suggests that intraneural tissue produces a highly reproducible pressure signature upon fluid injection.
- Intraneural Injection Was Detected After Only 0.2 mL
The pressure monitoring system detected an intraneural injection after an injection volume of only 0.2 mL.
At that point, the mean injection pressure had already risen to:
- 120 mm Hg
- Equivalent to approximately 2.3 PSI
This is an exceptionally small injected volume, suggesting that clinically meaningful pressure elevation occurs almost immediately after intraneural injection begins.
- Ultrasound Detected Swelling Later and Less Reliably
In contrast, ultrasound visualization of nerve swelling occurred:
- In only 10 of 12 injections (83%)
- At an average injected volume of 1.2 mL
This means pressure monitoring identified intraneural injection:
- Earlier
- More consistently
- At substantially lower injected volumes
Compared with ultrasound-based swelling detection.
Why These Findings Matter
This study directly challenges the assumption that ultrasound alone is the earliest warning system for intraneural injection.
Previous work by had suggested that ultrasound was superior to conventional in-line pressure monitors because ultrasound detected swelling at approximately 0.4 mL, whereas standard pressure systems using a 15 PSI threshold identified intraneural injection later and less reliably.
However, the current study argues that the limitation may not have been pressure monitoring itself, but rather the type of pressure monitoring being used.
Needle-Tip Pressure vs In-Line Pressure
Traditional in-line pressure monitors measure pressure at some point along the injection tubing system. Those measurements are affected by:
- Syringe characteristics
- Tubing compliance
- Needle length
- Needle diameter
- Injection speed
Needle-tip monitoring bypasses these confounders by measuring pressure directly at the tissue interface.
The authors argue that this provides a more physiologic and accurate representation of intraneural pressure.
A Potentially New Safety Threshold
One of the most provocative aspects of the study is the proposed reconsideration of safety thresholds for injection pressure.
Historically, many clinicians have used:
- 15 PSI (~776 mm Hg)
as a warning threshold for intraneural injection.
However, this study observed clear intraneural pressure elevation at only:
- 120 mm Hg
- 2.3 PSI
after merely 0.2 mL injection volume.
The authors, therefore, question whether the currently accepted thresholds are far too high.
If intraneural pressure rises substantially before reaching 15 PSI, waiting for that threshold may unnecessarily delay detection.
This raises important future research questions:
- What pressure truly predicts nerve injury?
- How long do elevated intraneural pressures persist?
- Is a lower “physiologic” safety threshold preferable?
- Could early micro-volume detection reduce neurologic complications?
Clinical Interpretation
Although this was a cadaveric study rather than a clinical outcomes trial, several practical messages emerge.
Ultrasound Alone May Not Be Enough
Ultrasound remains essential for regional anesthesia, but it is not infallible.
Needle visibility can be challenging in:
- Deep blocks
- Obese patients
- Poor acoustic windows
- Difficult anatomy
Furthermore, even when the needle is clearly visible, nerve swelling may not occur or be recognized immediately.
The current study reinforces that ultrasound should not be considered a standalone safety mechanism.
Multimodal Safety Remains Important
Modern regional anesthesia safety relies on combining multiple monitoring strategies:
- Ultrasound visualization
- Incremental injection
- Aspiration
- Patient feedback
- Low opening injection pressure
- Resistance monitoring
- Appropriate sedation levels
Needle-tip pressure monitoring could potentially become another valuable adjunct within this multimodal approach.
Earlier Detection Could Reduce Injury Severity
If clinicians can identify intraneural injection after only 0.2 mL rather than after 1–2 mL, this could theoretically:
- Reduce intraneural pressure exposure
- Minimize fascicular injury
- Lower ischemic damage risk
- Reduce neurologic complications
However, this remains speculative until validated in clinical studies.
Important Limitations
The authors appropriately acknowledge several limitations.
Cadaveric Model
Cadaver tissue does not perfectly replicate living human tissue.
Differences may exist in:
- Tissue compliance
- Elasticity
- Perfusion
- Pressure dissipation
Therefore, measured pressures may differ in vivo.
Small Sample Size
Only 12 injections were performed.
While the pressure findings were highly consistent, the sample size limits statistical power and generalizability.
Deliberate Intraneural Placement
The investigators intentionally created intraneural injections under idealized conditions.
Clinical practice involves variable anatomy, dynamic needle movement, and less controlled circumstances.
Clinical Injury Was Not Evaluated
The study did not assess:
- Histologic damage
- Functional nerve injury
- Neurologic outcomes
Thus, the exact relationship between pressure thresholds and clinical injury remains unknown.
Conclusion
This cadaveric study suggests that real-time continuous pressure monitoring directly at the needle tip may identify intraneural injection earlier and more consistently than ultrasound visualization of nerve swelling.
The findings challenge conventional assumptions about injection pressure thresholds and suggest that clinically relevant intraneural pressure elevations occur at far lower volumes and pressures than previously recognized.
While ultrasound remains indispensable for regional anesthesia, this study highlights the potential value of needle-tip pressure monitoring as an additional safety layer—particularly for detecting intraneural injection before visible sonographic changes develop.
Practical Tip
When performing peripheral nerve blocks, never rely on a single safety mechanism alone. NYSORA standard practice continues to recommend triple monitoring during peripheral nerve blocks to maximize patient safety:
- Ultrasound guidance for real-time needle and local anesthetic visualization
- Injection pressure monitoring to help detect high-resistance or potential intraneural injection
- Nerve stimulation to provide additional functional confirmation of needle proximity to neural structures
The combination of all three modalities may offer the safest approach, particularly in high-risk regional anesthesia procedures.
For more information, refer to the full article in RAPM.
Dossi R, Quadri C, Capdevila X, Saporito A. Real time continuous monitoring of injection pressure at the needle tip is better than ultrasound in early detecting intraneural injection. Reg Anesth Pain Med. 2026 Apr 2;51(4):460-464.
Read more about injection pressure monitoring in our Regional Anesthesiology Module on NYSORA 360 on NYSORA360 – an essential learning resource for residents with practical, up-to-date guidance.