Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About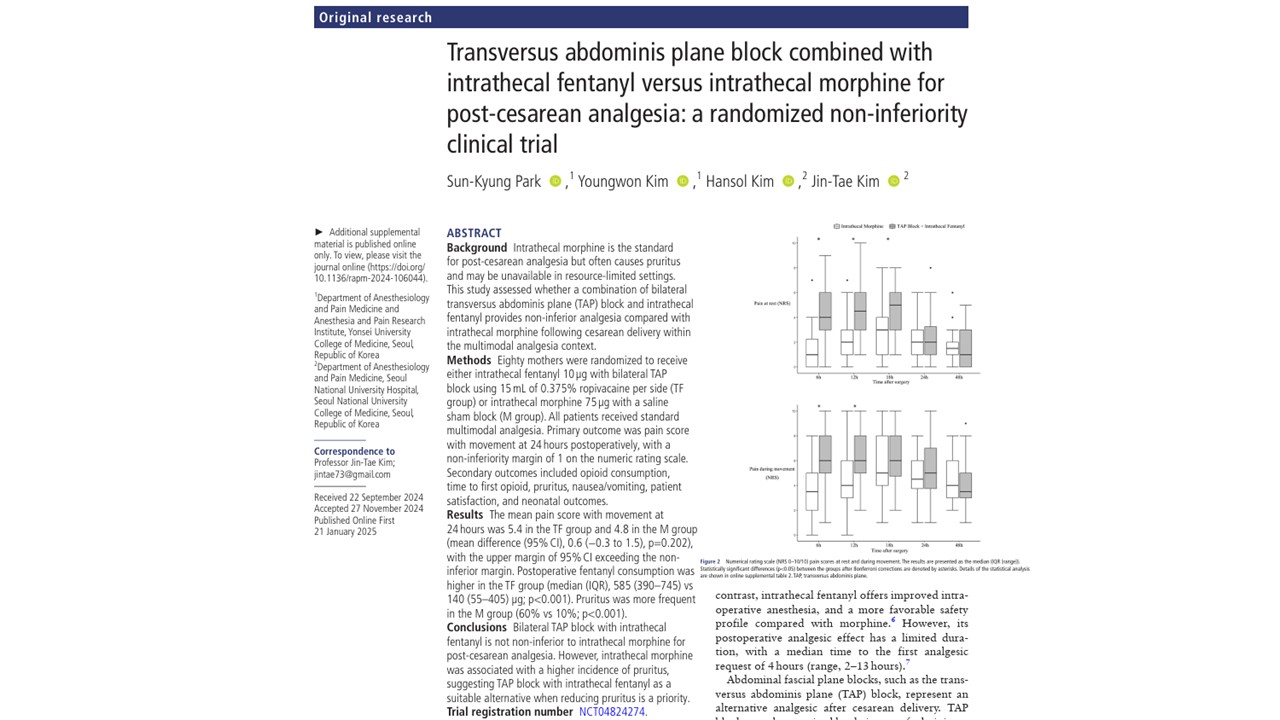





Effective postoperative analgesia following cesarean delivery is essential for optimizing maternal recovery, facilitating early ambulation, promoting breastfeeding, and reducing postoperative morbidity. Neuraxial anesthesia—particularly spinal anesthesia with adjunct opioids—remains the cornerstone of cesarean section analgesia.
Among available options, intrathecal morphine has long been considered the gold standard due to its potent and prolonged analgesic properties. However, its clinical use is frequently complicated by opioid-related adverse effects, most notably pruritus, nausea, and the potential for delayed respiratory depression.
A newly published randomized, double-blind, non-inferiority clinical trial in RAPM provides critical insights into whether a combination of bilateral transversus abdominis plane (TAP) block and intrathecal fentanyl can serve as a viable alternative. The findings ultimately reinforce the continued dominance of intrathecal morphine while highlighting clinically meaningful trade-offs in side-effect profiles.
Background
Post-cesarean pain is multifactorial, involving both somatic and visceral components:
- Somatic pain arises from abdominal wall incision and tissue trauma
- Visceral pain originates from uterine manipulation and contraction
Intrathecal morphine is uniquely effective because it addresses both components through central opioid receptor activation. However, its pharmacodynamic profile also explains its adverse effects.
Key challenges with intrathecal morphine
- High incidence of opioid-induced pruritus (reported up to 70–90%)
- Risk of delayed respiratory depression due to cephalad spread in cerebrospinal fluid
- Requirement for postoperative respiratory monitoring
- Limited availability in certain healthcare settings
These limitations have driven interest in multimodal and regional techniques, particularly fascial plane blocks such as the TAP block.
Study objective and hypothesis
The trial aimed to determine whether a combined approach—intrathecal fentanyl plus bilateral TAP block—could provide non-inferior analgesia compared with intrathecal morphine within a multimodal analgesic regimen.
Hypothesis
- TAP block + fentanyl would provide comparable pain relief
- The combination would reduce opioid-related side effects
- Overall, patient experience might improve despite differences in analgesic potency
Study design and methodology
- Design: randomized, double-blind, non-inferiority trial
- Sample size: 80 patients (40 per group)
- Population: healthy women undergoing elective cesarean delivery under spinal anesthesia
- Setting: tertiary academic medical center
Intervention groups
Group 1: TAP + fentanyl (TF group)
- Intrathecal fentanyl 10 µg
- Bilateral TAP block with 0.375% ropivacaine (15 mL per side)
Group 2: Morphine (M group)
- Intrathecal morphine 75 µg
- Sham TAP block (saline)
Multimodal analgesia protocol
All patients received:
- Intravenous acetaminophen
- Scheduled oral acetaminophen
- Non-steroidal anti-inflammatory drugs (NSAIDs)
- Intravenous patient-controlled analgesia (PCA) with fentanyl
This standardized regimen ensured that differences observed were attributable to the primary interventions.
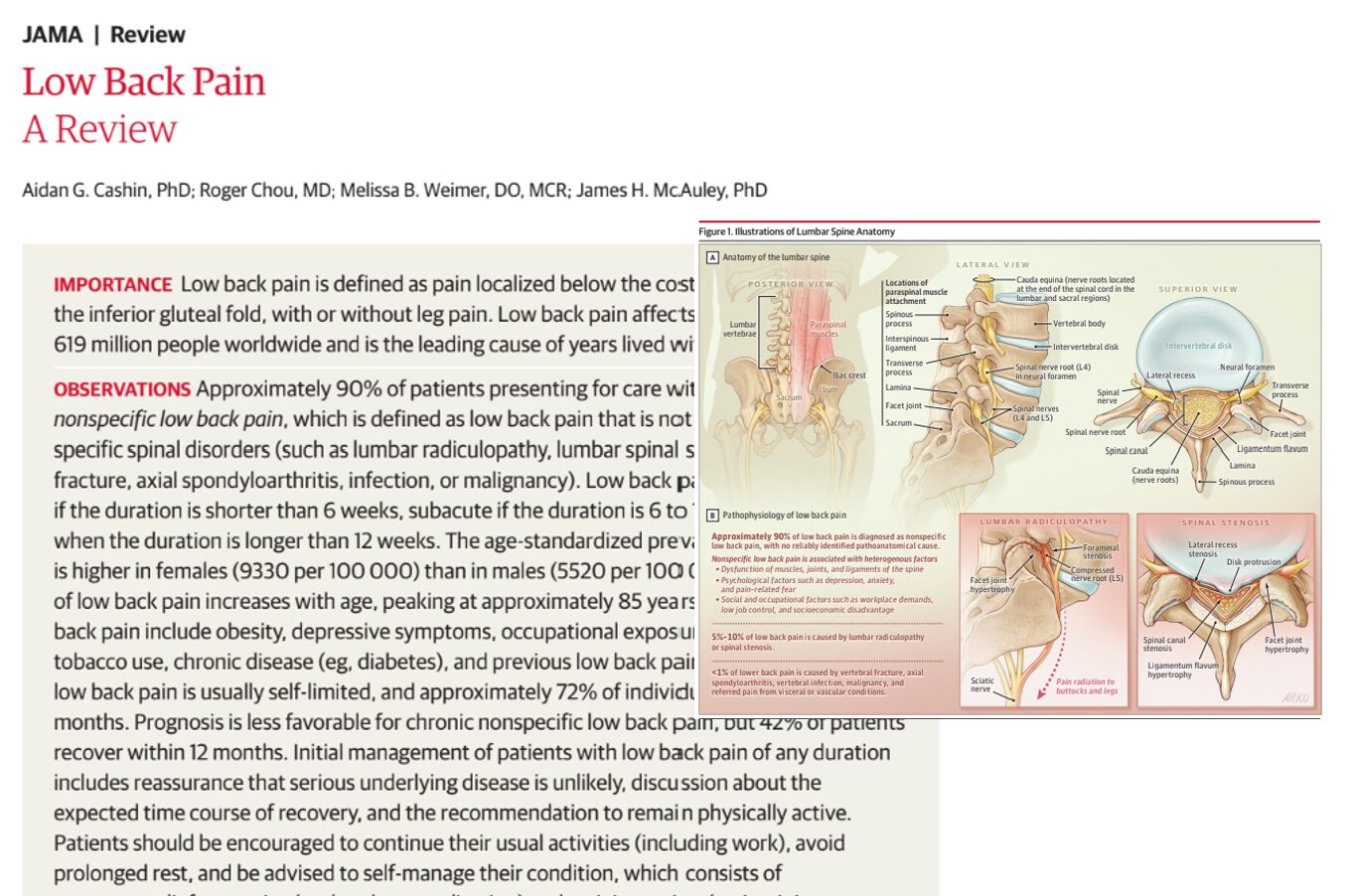
Understanding the TAP block technique
The TAP block is a regional anesthesia technique targeting thoracolumbar nerves (T6–L1) within the fascial plane between the internal oblique and transversus abdominis muscles.
Physiological mechanism
- Local anesthetic diffuses within the fascial plane
- Blocks afferent somatic nerve transmission
- Reduces incisional pain without affecting visceral nociception
Procedural steps
- Position the ultrasound transducer along the midaxillary line
- Identify abdominal muscle layers
- Advance needle using the in-plane technique
- Confirm placement via hydrodissection
- Inject local anesthetic bilaterally
While effective for somatic pain, the TAP block does not adequately address visceral pain, which may explain differences in analgesic outcomes.
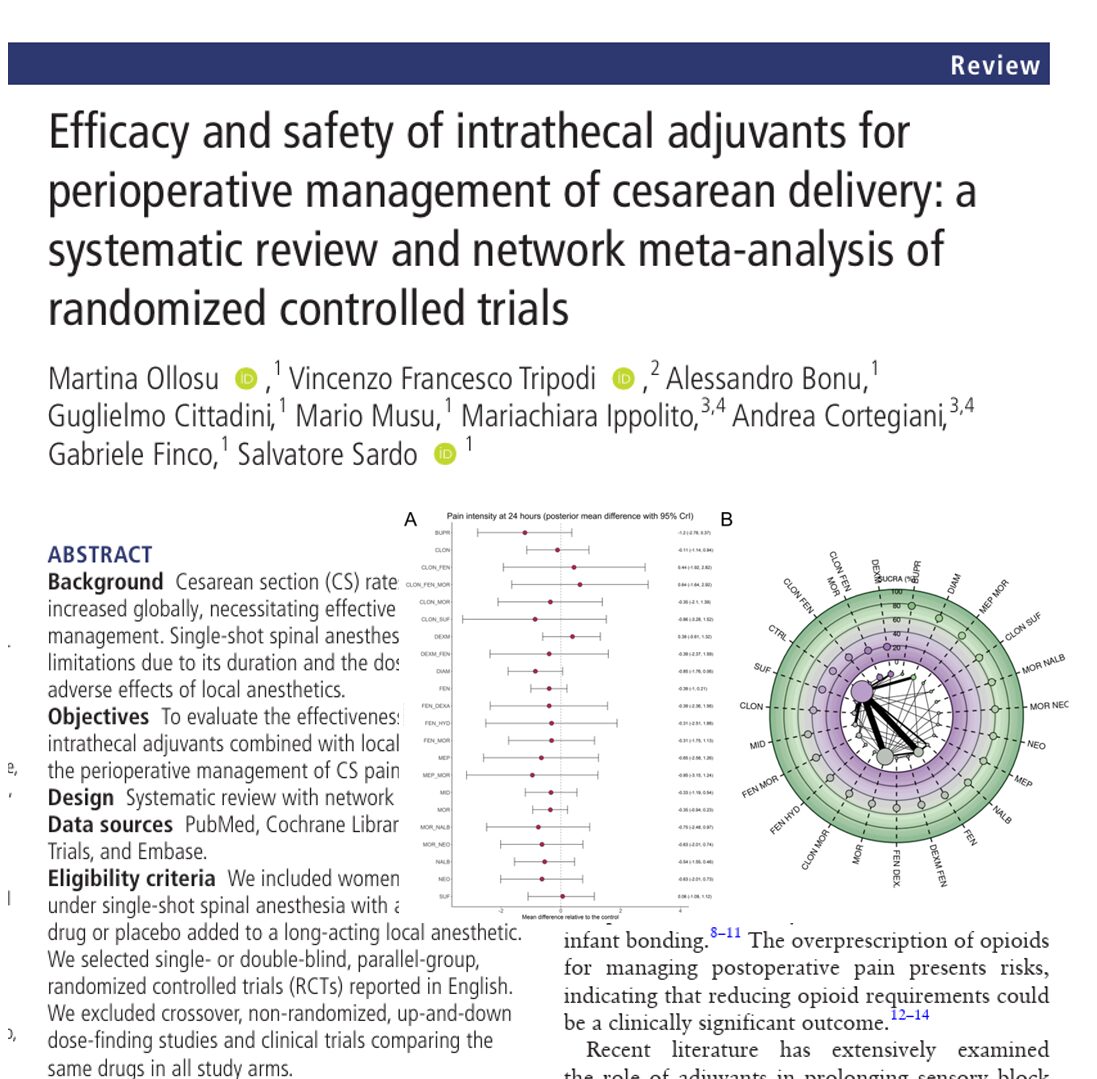
Primary outcome: pain during movement at 24 hours
The primary endpoint was pain intensity during movement at 24 hours postoperatively, measured using the numeric rating scale (NRS).
Results
- TAP + fentanyl: mean NRS 5.4
- Morphine: mean NRS 4.8
- Mean difference: 0.6 (95% CI −0.3 to 1.5)
The predefined non-inferiority margin was 1 point on the NRS.
Interpretation
- The upper bound of the confidence interval exceeded the margin
- Non-inferiority was not demonstrated
This indicates that the TAP block combined with fentanyl does not provide analgesia equivalent to intrathecal morphine.
Opioid consumption
Postoperative opioid requirements were significantly higher in the TAP + fentanyl group.
- Median fentanyl consumption:
- TAP + fentanyl: 585 µg
- Morphine: 140 µg
This reflects:
- Shorter duration of analgesia with fentanyl
- Insufficient coverage by the TAP block alone
Time to first analgesic request
- TAP + fentanyl: 11.6 hours
- Morphine: 16.8 hours
Intrathecal morphine provided prolonged analgesia, delaying the need for rescue medication.
Pain trajectory over time
According to the pain score graph on page 3, the TAP + fentanyl group exhibited:
- Higher pain scores at rest up to 18 hours
- Higher pain scores during movement up to 12 hours
This demonstrates a consistent early postoperative disadvantage compared with morphine.
Rescue analgesia requirements
- The TAP + fentanyl group had significantly higher use of rescue medications
- Increased reliance on ketoprofen and propacetamol
This further supports inferior analgesic efficacy.
Pruritus
- Morphine group: 60%
- TAP + fentanyl group: 10%
This represents a sixfold increase in pruritus with morphine.
Clinical significance
- Pruritus can significantly affect patient comfort
- Often requires pharmacologic intervention (e.g., ondansetron, nalbuphine)
Respiratory depression
- No cases in the morphine group
- One case in the TAP + fentanyl group
The affected patient responded well to naloxone and supportive care.
Nausea and vomiting
- No significant difference between groups
Patient satisfaction
Despite differences in pain and side effects:
- Satisfaction scores were similar
- Sleep quality did not differ significantly
This suggests that overall patient perception is influenced by multiple factors beyond pain intensity.
Neonatal outcomes
Neonatal safety is a critical consideration in obstetric anesthesia.
Findings
- No differences in Apgar scores
- No differences in umbilical arterial blood gas analysis
This confirms that both analgesic approaches are neonatally safe.
Clinical interpretation: balancing efficacy and tolerability
The study highlights a fundamental principle in anesthesiology:
Optimal analgesia requires balancing efficacy with side-effect burden.
Advantages of intrathecal morphine
- Superior analgesic efficacy
- Longer duration of action
- Reduced need for additional opioids
Disadvantages
- High incidence of pruritus
- Need for monitoring
Advantages of TAP + fentanyl
- Lower incidence of pruritus
- Favorable safety profile
- Useful when morphine is unavailable
Disadvantages
- Inferior pain control
- Higher opioid consumption
- Shorter analgesic duration
Implications for clinical practice
Recommended approach
Intrathecal morphine should remain the first-line agent for post-cesarean analgesia when:
- Monitoring resources are available
- Patients tolerate opioids
- Maximizing analgesic efficacy is the priority
Alternative strategy
TAP block with intrathecal fentanyl may be considered when:
- Pruritus is a major concern
- Morphine is contraindicated or unavailable
- Opioid minimization is desired
Study limitations
- Single-center design limits generalizability
- Lack of sensory confirmation of TAP block success
- Fixed dosing may not reflect optimal regimens
- Primary outcome timing may disadvantage fentanyl
Future directions
Further research should focus on:
- Combining multiple regional techniques
- Optimizing opioid dosing strategies
- Exploring novel analgesics with improved side-effect profiles
- Developing individualized pain management protocols
Conclusion
This randomized clinical trial reinforces the clinical superiority of intrathecal morphine for post-cesarean analgesia within a multimodal framework. While the TAP block combined with intrathecal fentanyl offers a reduced incidence of pruritus, it fails to achieve comparable analgesic efficacy.
Ultimately, the choice of analgesic strategy should be individualized, taking into account patient preferences, institutional resources, and the relative importance of pain control versus side-effect reduction.
The findings underscore a critical reality in obstetric anesthesia: no single approach is universally optimal, and the pursuit of balanced, patient-centered analgesia must continue.
For more information, refer to the full article in RAPM.
Park SK, Kim Y, Kim H, Kim JT. Transversus abdominis plane block combined with intrathecal fentanyl versus intrathecal morphine for post-cesarean analgesia: a randomized non-inferiority clinical trial. Reg Anesth Pain Med. 2026 Mar 5;51(3):330-336.
Download the Nerve Blocks App HERE for step-by-step guidance on the TAP block. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Module on NYSORA360!