Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About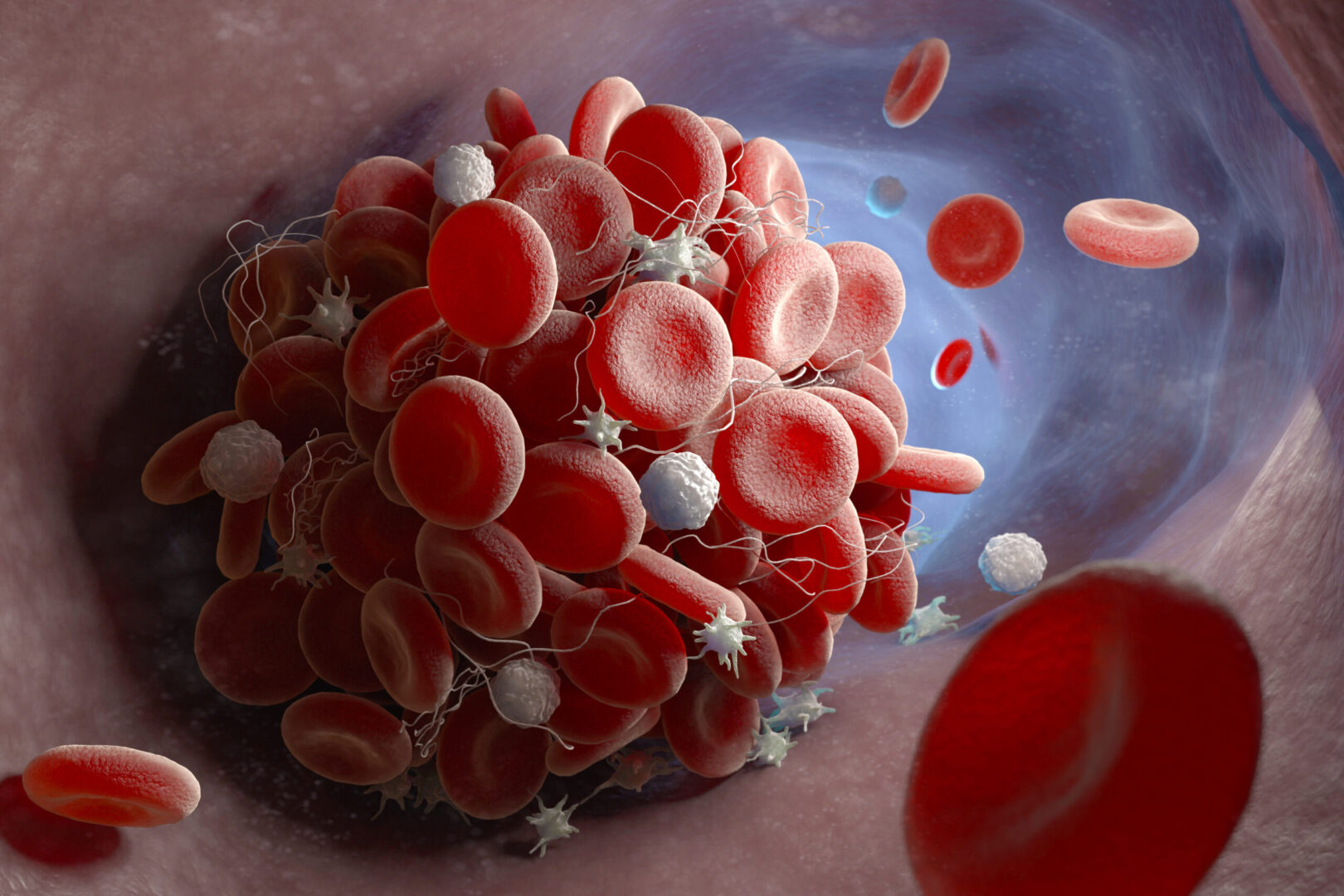
Learning objectives
- Describe the mechanisms and risk factors for venous thromboembolism
- Prevent perioperative venous thromboembolism
- Diagnose and manage venous thromboembolism
Background
- Venous thromboembolism (VTE) is a major cause of morbidity and mortality in both hospital and community settings
- Most preventable cause of mortality in hospitalized patients
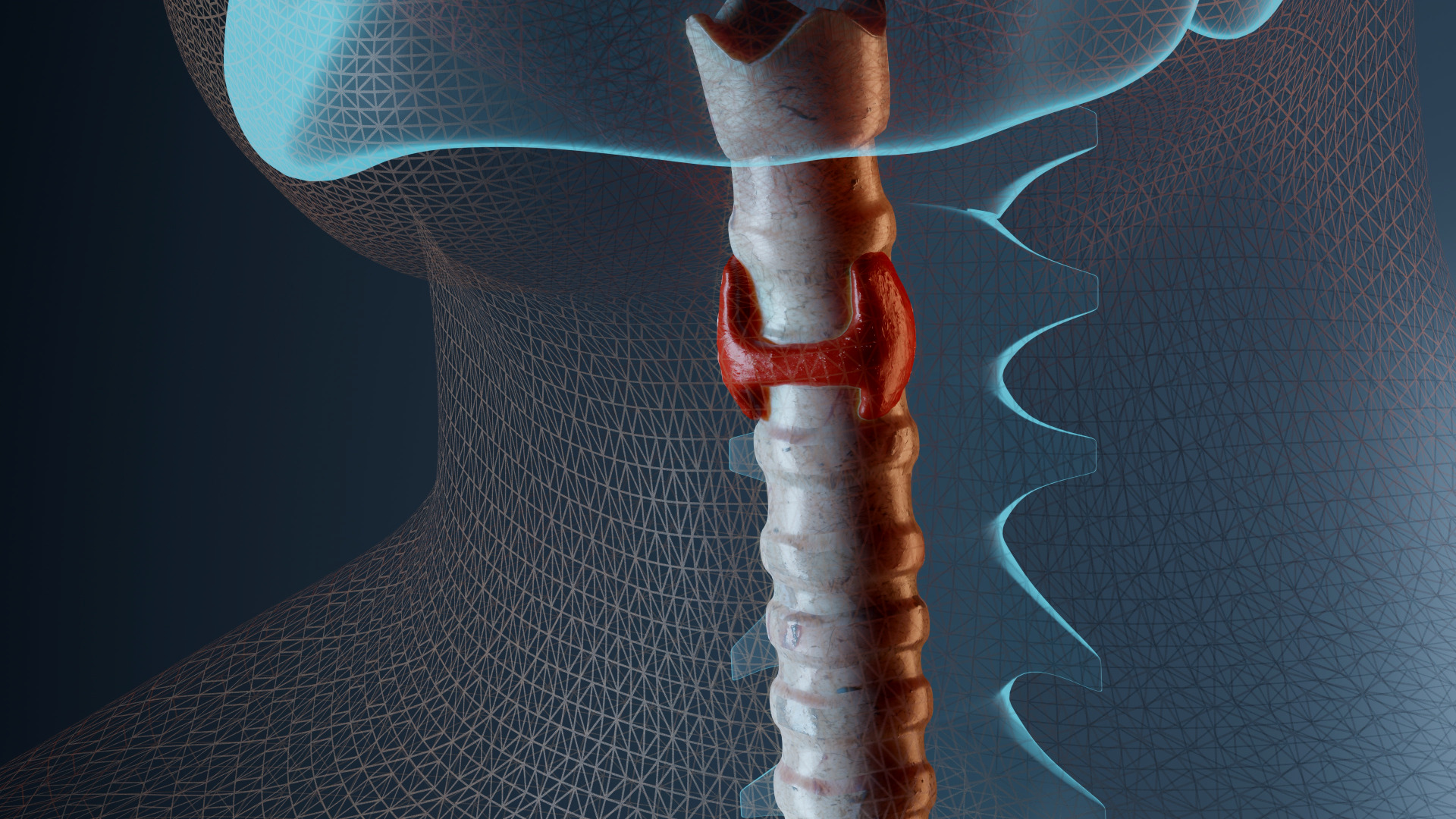
- Encompasses deep vein thrombosis (DVT) and pulmonary embolism (PE)
- DVT occurs when red blood cells, fibrin, platelets, and leucocytes form a mass within an intact deep vein
- Signs & symptoms are nonspecific and only occur in up to 50% of patients
- PE occurs in about a third of patients with a DVT
- Adequate perioperative thromboprophylaxis is essential to prevent perioperative VTE
Risk factors
- Three main factors that cause thrombosis:
- Alterations in blood flow (stasis and turbulence)
- Vascular endothelial injury
- Alterations in the blood coagulability
- Risk factors:
| Stasis–endothelial injury | Thrombophilias | Medical conditions | Medications | Other |
|---|---|---|---|---|
| Indwelling venous device | Activated protein C resistance | Malignancy (solid tumour and myeloproliferative disorders) | Oral contraceptive use (combined only) | Increasing age |
| Surgery (abdominal, pelvic, orthopedic most commonly) | Factor V Leiden | Pregnancy, postpartum | Hormone replacement therapy | Smoking |
| Major trauma, burns | Prothrombin gene mutation G20210A | Myocardial infarction | Chemotherapy (including tamoxifen) | |
| Prolonged travel | Hyperhomocysteinemia | Congestive heart failure | ||
| Paralysis (including anesthesia for >30 min) | Anticardiolipin antibodies | Obesity | ||
| Varicose veins | Lupus anticoagulant | Inflammatory bowel disease | ||
| Elevated factor VIII level | Nephrotic syndrome | |||
| Protein C deficiency | History of VTE | |||
| Protein S deficiency | Heparin-induced thrombocytopenia | |||
| Dysfibrinogenemia | Paroxysmal nocturnal hemoglobinuria | |||
| Dysplasminogenemia | ||||
| Antithrombin deficiency |
Pathophysiology
- Venous thrombi typically develop at a site of vascular trauma, around intravascular catheters, or in areas of reduced blood flow (e.g., venous valves)
- Accumulation of fibrin and platelets causes rapid growth in the direction of blood flow
- Endogenous fibrinolysis results in partial or complete resolution of the thrombus
- Any residual thrombus may result in incomplete recanalization of the vein, potentially narrowing the lumen and causing valve incompetence
- Extensive collateral network may develop
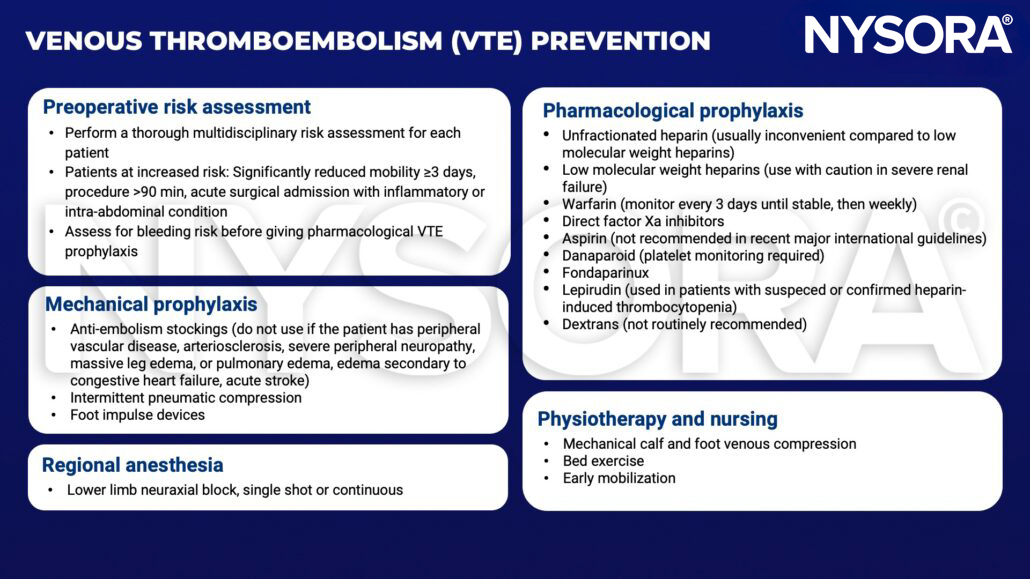
Prevention
Diagnosis
- DVT
- Duplex ultrasonography
- D-dimer blood test
- Contrast venography
- MRI
- PE
- Computed tomographic pulmonary angiography
- Ventilation-perfusion scan
- Pulmonary angiography
- MRI
Management
- Preferred DVT treatment: Low molecular weight heparins
- Maintain anticoagulation for 3-6 months for VTE secondary to transient risk factors and >12 months for recurrent VTE
- Thrombolytics in severe cases
- When anticoagulation fails: Inferior vena cava filter
- Thrombectomy/embolectomy (rarely required)
Suggested reading
- Gordon RJ, Lombard FW. Perioperative Venous Thromboembolism: A Review. Anesthesia & Analgesia. 2017;125(2).
- Barker RC, Marval P. Venous thromboembolism: risks and prevention. Continuing Education in Anaesthesia Critical Care & Pain. 2011;11(1):18-23.
- National Clinical Guideline Centre – Acute and Chronic Conditions (UK). Venous Thromboembolism: Reducing the Risk of Venous Thromboembolism (Deep Vein Thrombosis and Pulmonary Embolism) in Patients Admitted to Hospital. London: Royal College of Physicians (UK); 2010. (NICE Clinical Guidelines, No. 92.) 2, Summary of recommendations. Available from: https://www.ncbi.nlm.nih.gov/books/NBK116536/
Clinical updates
Romero et al. (EJA, 2024), on behalf of the European Society of Anaesthesiology and Intensive Care, report the first major update since 2018 of European peri-operative VTE prophylaxis guidelines, expanding recommendations to new specialties (plastic surgery, urology, trauma, and non-ambulatory orthopedics) and emphasizing individualized risk assessment using tools such as the Caprini score. Key changes include stronger endorsement of combined mechanical (IPC) and pharmacological prophylaxis for high-risk patients (e.g., obese and bariatric surgery patients with higher-dose LMWH), earlier but carefully timed postoperative anticoagulation in cardiac and neurosurgery, and extended prophylaxis (≥ 7 days, up to 4 weeks) after major orthopedic surgery. The guidelines also prioritize early mobilization and hydration in low-risk fast-track surgery, and recommend postoperative initiation of LMWH when neuraxial anesthesia is used to reduce spinal hematoma risk.
- Read more about this study HERE.