Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About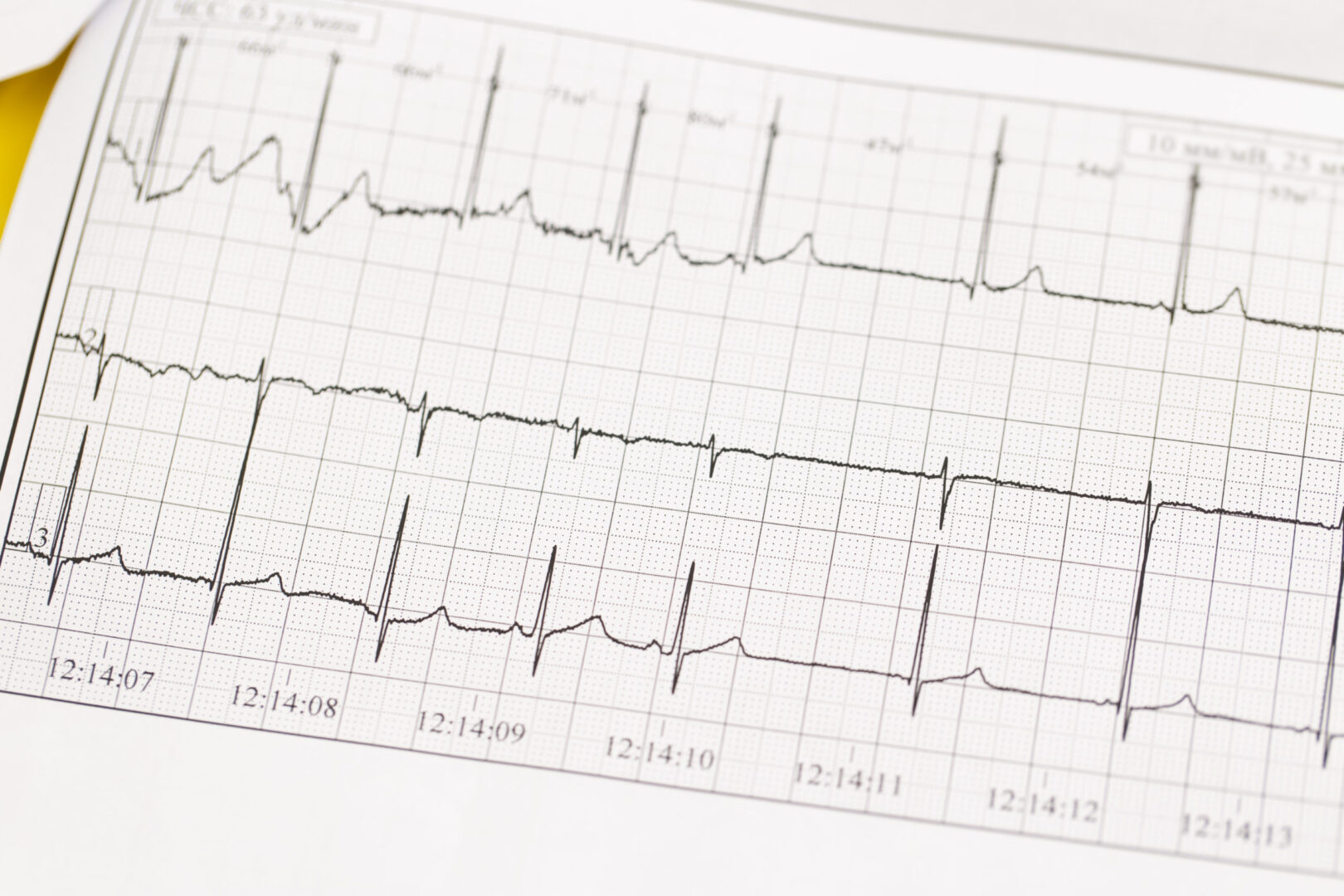
Learning objectives
- Definition, diagnosis, and management of hyperkalemia
Definition
- Hyperkalemia is an elevated level of potassium (K+) in the blood:
- Mild: a serum K+ 5.5 – 5.9 mmol/L
- Moderate: a serum K+6.0-6.4 mmol/L
- Severe: a serum K+ ≥ 6.5 mmol/L
Signs and symptoms
- Gastro-intestinal
- Nausea
- Vomiting
- Diarrhea
- Neuromuscular
- Paresthesias
- Muscle fasciculations
- Ascending paralysis of the extremities (quadriplegia)
- Cardiac
- Dyspnea
- Progressive ECG changes with increasing severity of hyperkalemia
- Peaked T wave
- Wide PR interval
- Wide QRS duration
- Loss of P wave
- Sinusoidal wave
Causes
| Renal failure | |
| Medications | Angiotensin-converting enzyme inhibitors (ACE-i) Angiotensin II receptor blockers (ARB) Potassium-sparing diuretics Non-steroidal anti-inflammatory drugs (NSAIDs) Beta-blockers Trimethoprim (antibiotic) |
| Tissue breakdown | Rhabdomyolysis Trauma |
| Endocrine disorders | Diabetes mellitus type 2 Adrenocortical insufficiency |
Management
- First, ensure that the lab result is correct and rule out pseudohyperkalemia
- Typical examples:
- Poor storage of blood specimens
- Long transport time from blood draw of the sample to processing in the lab

Suggested reading
- Lott C, Truhlář A, Alfonzo A, et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances [published correction appears in Resuscitation. 2021 Oct;167:91-92]. Resuscitation. 2021;161:152-219.
- Palmer BF, Carrero JJ, Clegg DJ, et al. Clinical Management of Hyperkalemia. Mayo Clin Proc. 2021;96(3):744-762.
- Palmer BF, Clegg DJ. Diagnosis and treatment of hyperkalemia. Cleve Clin J Med. 2017;84(12):934-942. doi:10.3949/ccjm.84a.17056
Clinical updates
Jessen et al. (Resuscitation, 2025) conducted a systematic review and meta-analysis showing that insulin with glucose lowers serum potassium by about 0.7 mmol/L within 60 minutes, while inhaled or IV beta₂-agonists (e.g., salbutamol) reduce potassium by 0.9–1.0 mmol/L, with combination therapy achieving up to a 1.2 mmol/L reduction. In contrast, bicarbonate showed no meaningful potassium-lowering effect, and there is no high-quality evidence that calcium improves outcomes beyond membrane stabilization. These findings support insulin–glucose and beta₂-agonists as first-line therapies for acute hyperkalemia and call for re-evaluation of routine bicarbonate and calcium use.
Glahn et al. (British Journal of Anaesthesia, 2025) highlight in the updated 2024 EMHG guidelines that severe hyperkalemia is a key life-threatening feature of malignant hyperthermia (MH) and requires immediate treatment alongside dantrolene. Recommended management includes IV insulin with dextrose, IV calcium chloride or gluconate for membrane stabilization, beta₂-agonists, and dialysis in refractory cases, with close potassium and ECG monitoring. The guideline reinforces structured, protocol-driven hyperkalemia treatment as a core component of MH crisis management to prevent arrhythmias and cardiac arrest.
- Read more about this study HERE.