Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Involved systems in and classification of amyloidosis
- Anesthetic management of amyloidosis
Definition and mechanisms
- Amyloidosis constitutes a group of diseases characterized by the extracellular deposition of insoluble protein aggregates
- Precursor proteins, produced by various mechanisms, are deposited extracellularly as insoluble fibrils resulting in disruption of tissue architecture and organ dysfunction
- The disease spectrum may be inherited or acquired and localized or systemic
- May occur as its own entity or in association with dialysis-dependent renal failure, chronic infection, or inflammation
- Diagnosed based on histological demonstration of amyloid deposits in affected tissues
Classification of amyloid subtypes
| Abbreviation | Protein type | Major Anaesthetic Considerations | Treatment |
|---|---|---|---|
| AL | Light chain (plasma cell-derived) | Airway difficulties, cardiomyopathy, arrhythmias, renal failure, hepatic failure, bleeding, autonomic/peripheral neuropathy, endocrine organ dysfunction, treatment-related complications | Symptomatic, chemotherapy, immunosuppression, endocrine supplementation, stem cell/organ transplantation |
| AA | Serum amyloid A (acute phase protein) | Features of underlying cause: Infection: TB, leprosy, Bronchiectasis Inflammation Autoimmune disease Malignancy: Hodgkin’s lymphoma Respiratory tract lesions Hepatic failure Renal failure Treatment-related complications | Treat underlying cause, surgical (localized disease) |
| Ab | b-Amyloid | Consent issues (Alzheimer’s dementia) | Supportive |
| Ab2M | b2-Microglobulin | Dialysis-dependent renal failure, difficult positioning (arthropathy) | Symptomatic, renal transplant |
| ATTR | Transthyretin Wild type (‘Senile’) Mutant type (Hereditary) | Heart failure (males, slow progressive) Autonomic/peripheral neuropathy, cardiomyopathy, gastrointestinal dysfunction | Symptomatic Symptomatic, liver transplant |
Systems involved
| Associated complications | |
|---|---|
| Airway and the respiratory system | Failed intubation Hemorrhage Obstruction Macroglossia predisposes to difficult intubation Laryngeal amyloid presents with hoarseness, dyspnea, cough, stridor, and odynophagia Tracheobronchial involvement is relatively uncommon Parenchymal amyloid may be unilateral or bilateral, diffuse or nodular |
| Cardiovascular system | Restrictive cardiomyopathy Diastolic heart failure Conduction disorders Ischaemic heart disease Arrhythmias Orthostatic hypotension Congestive heart failure |
| Hematological system | Microvascular fragility Platelet dysfunction Impaired fibrin formation Clotting factor deficiencies: factor X is most common, factors II, VI, VII, and IX also reported Impaired vasoconstriction Increased risk of hemorrhage |
| Neurological system | Autonomic and peripheral neuropathy |
| Other systems | Renal dysfunction: nephrotic syndrome & renal failure Visceral organomegalyy Early satiety Malabsorption Protein-losing enteropathy Ascites Dysmotility Gastrointestinal hemorrhage Deranged liver function Thyroid, adrenals, and testes infiltration |
Anesthetic drugs in amyloidosis
| Class of drug | Caution |
|---|---|
| Anticholinergics | Blunted, or absent response |
| Anticoagulants | Use is contentious if bleeding risk evident |
| Benzylisoquinoliniums | Effect antagonized by anticholinesterase inhibitors |
| b-Blockers, Ca-channel blockers | Negative inotropic effects risk cardiac decompensation |
| Cardiac glycosides | Drug binding to protein fibrils risks toxicity at therapeutic levels |
| Depolarizing neuromuscular blocking agents | Potential for hyperkalaemic response in neurological dysfunction Prolonged action with anticholinesterase inhibitors |
| Halogenated volatile agents | Exposure increases in b-amyloid deposition in animal models |
| I.V. sedatives | Predictable haemodynamic depressant effects (except ketamine) Increased b-amyloid deposition not demonstrated with propofol, barbiturates and benzodiazepines |
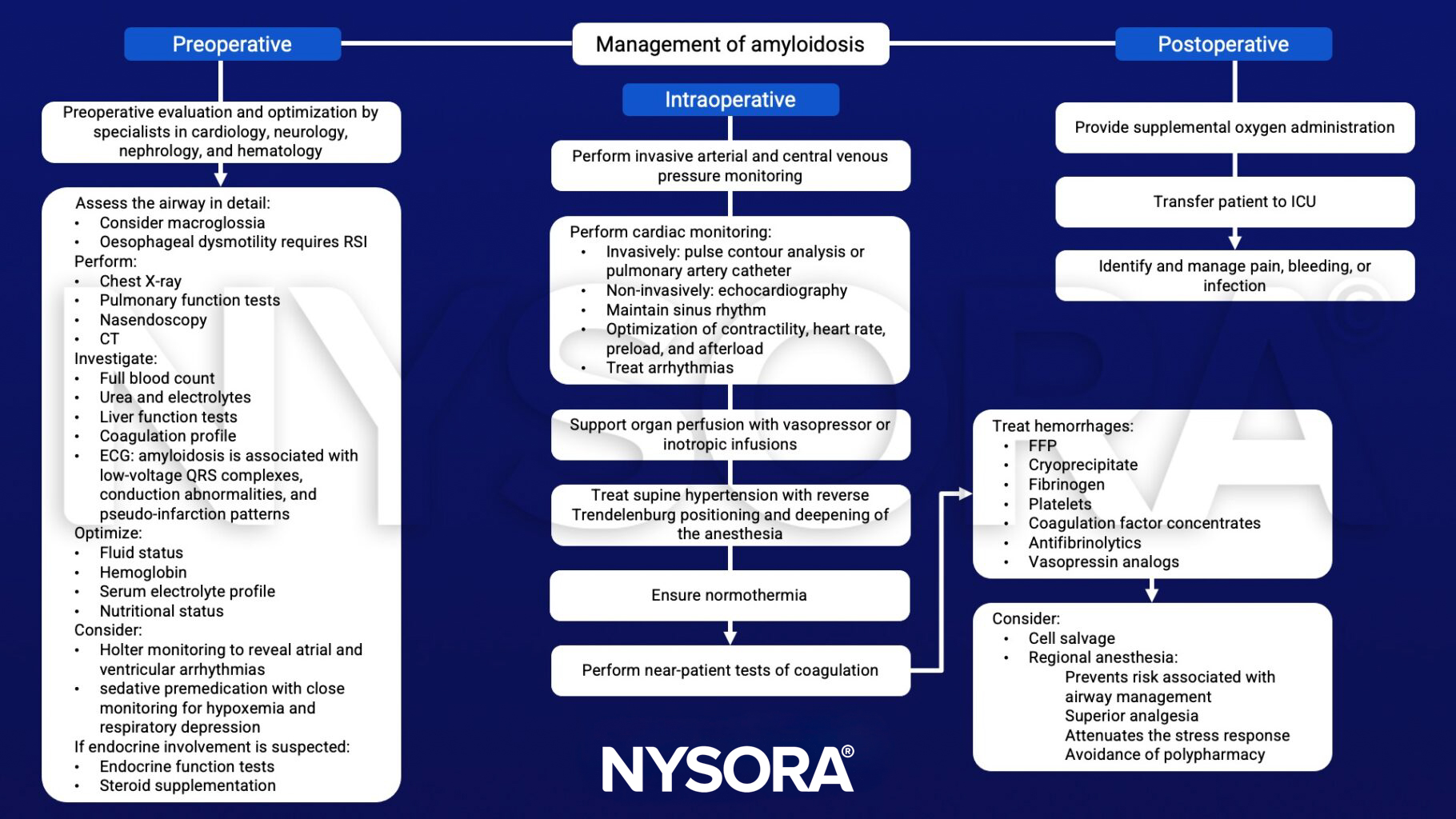
Management
Suggested reading
- Wani Z, Harkawat DK, Sharma M. Amyloidosis and Anesthesia. Anesth Essays Res. 2017;11(1):233-237.
- Fleming I, Dubrey S, Williams B. 2012. Amyloidosis and anaesthesia, Continuing Education in Anaesthesia Critical Care & Pain.12;(2);72–77.