Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Recognize chronic kidney disease (CKD)
- Management of CKD
Definition and mechanisms
- A slow and gradual loss of kidney function over a period of months to years
- Retention of fluid and waste products
- Can get worse over time and may lead to kidney failure
Signs & symptoms
Few symptoms in the early stages of CKD
- Nausea
- Vomiting
- Loss of appetite
- Fatigue
- Sleep problems
- Increased or decreased urination
- Headaches
- Muscle cramps
- Swelling of feet and ankles
- Dry, itchy skin
- Hypertension
- Shortness of breath
- Chest pain
- Weight loss
- Blood in urine
Stages of CKD
| CKD stage | eGFR (ml/min/1.73m²) | Description |
|---|---|---|
| 1 | >90 | Kidney damage with normal GFR |
| 2 | 60-89 | Kidney damage with mildly decreased GFR |
| 3 | 30-59 | Moderately decreased GFR |
| 4 | 15-29 | Severly decreased GFR |
| 5 | <15 | Kidney failure |
Causes
- Hypertension
- Diabetes
- High cholesterol
- Kidney infection
- Glomerulonephritis
- Polycystic kidney disease
- Heart disease/failure
- Longterm regular use of lithium or NSAIDs
Complications
| System | Effects |
|---|---|
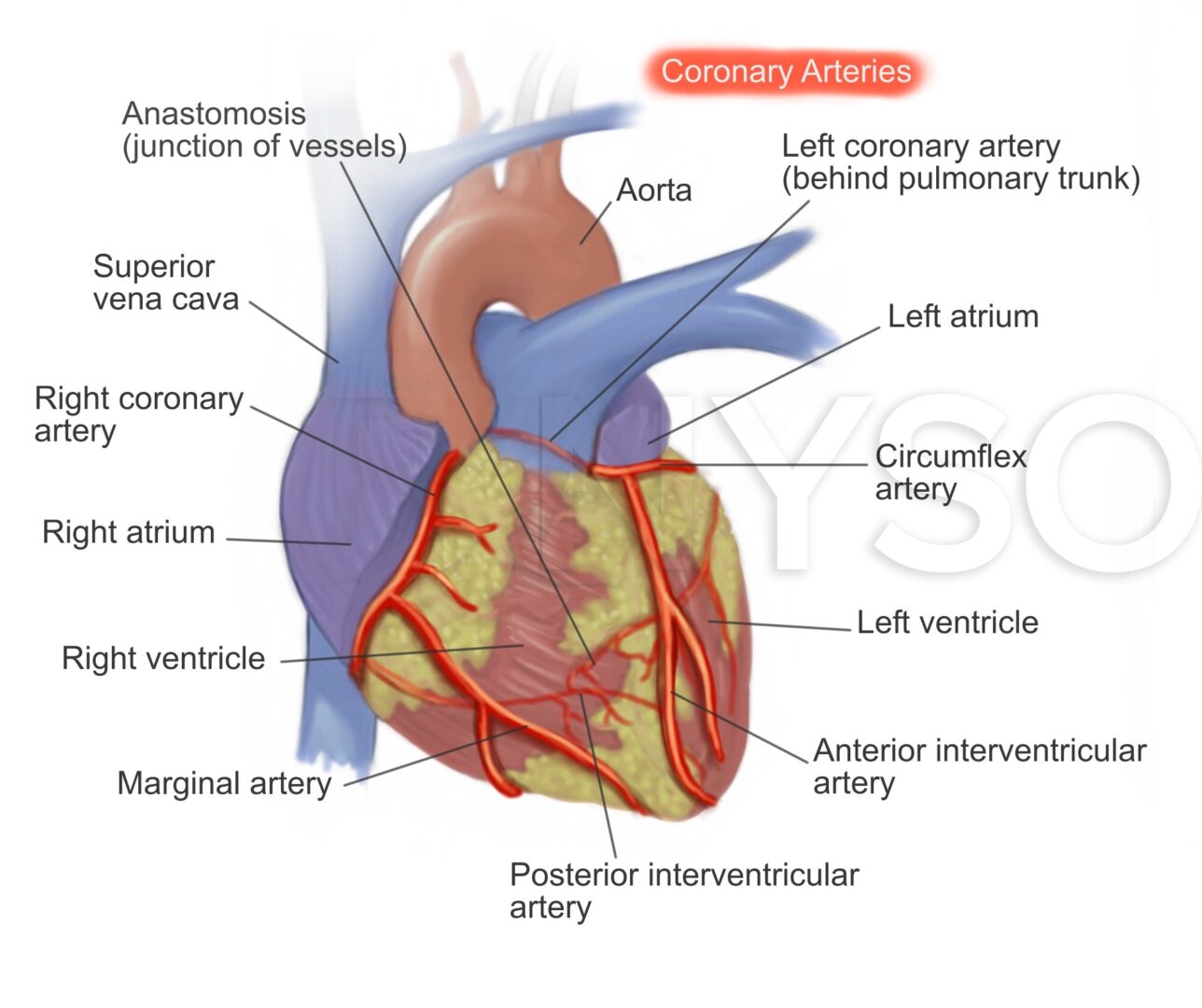
| Cardiovascular system | Hypertension Ischemic heart disease Pericarditis Heart failure |
| Respiratory system | Pulmonary edema Pleural effusion Respiratory infection |
| Central nervous system | Autonomic neuropathy Coma |
| Hematological | Perioperative anemia Bleeding tendency |
| Gastro-intestinal | Stress ulcertion Delayed gastric emptying |
| Renal and metabolic | Fluid retention Hyperkalemia Metabolic acidosis |
| Immunological aspects | Immunosuppressant |
Management
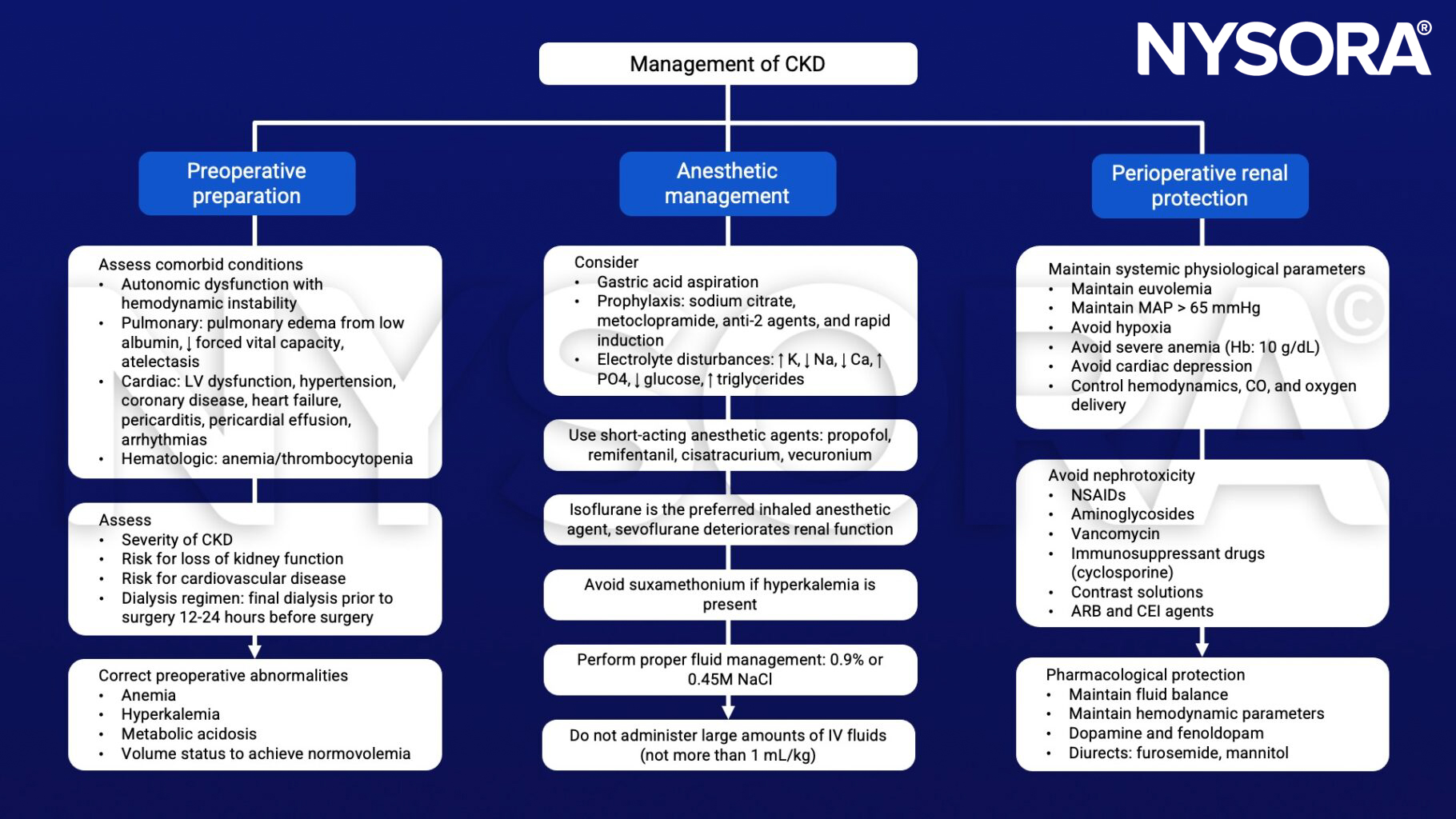
Keep in mind
- Decreased renal function can prolong anesthetic drug effects by decreased elimination of these agents
Suggested reading
- Domi R, Huti G, Sula H, et al. From Pre-Existing Renal Failure to Perioperative Renal Protection: The Anesthesiologist’s Dilemmas. Anesth Pain Med. 2016;6(3):e32386. Published 2016 May 14.
- Sladen RN. Chronic kidney disease: the silent enemy?. Anesth Analg. 2011;112(6):1277-1279.
Clinical updates
Herrington et al. (The Lancet, 2026) synthesize post-2019 trial evidence into an updated “standard of care” bundle for CKD that targets both kidney failure and cardiovascular risk: SGLT2 inhibitors, RAS inhibition, statin-based regimens, and intensive blood pressure targets as core interventions, with GLP-1 receptor agonists and finerenone added for CKD with type 2 diabetes where appropriate. A key update is the strong emphasis on the implementability of these treatments across many clinical settings and on the potential for broad uptake to substantially reduce the global complication burden of CKD.
Georgakis et al. (Anesthesia & Analgesia, 2025) report that, in a propensity-matched CKD cohort, rocuronium + sugammadex was associated with higher short-term cardiopulmonary complications versus cisatracurium + neostigmine—including respiratory failure, acute respiratory distress, hypertensive crisis, heart failure, pleural effusion, and 30-day mortality. These findings suggest that, in patients with CKD, selecting an organ-independent NMBA (cisatracurium) may be a safer default when clinically feasible, pending prospective confirmation.
Grams & Melamed (Annals of Internal Medicine, 2025) emphasize a more proactive, therapy-enabled screening approach: because effective kidney-protective drugs now exist, they recommend screening at-risk patients with serum creatinine (± cystatin C) and urine ACR, with annual screening clearly for diabetes and more broadly (but more controversially) for hypertension/CVD/older adults. Therapeutically, they highlight newer disease-modifying options beyond ACEi/ARB—e.g., GLP-1 receptor agonist data and finerenone as an add-on in diabetic CKD with residual albuminuria despite ACEi/ARB.
Renberg et al. (British Journal of Anaesthesia, 2024) found that advanced CKD (eGFR <30) within 1 year of noncardiac surgery was uncommon in patients without known preoperative renal dysfunction (0.67%), but major adverse kidney events (MAKE365: eGFR <30, dialysis, or death) occurred in 7.1%. The key new signal is that advanced AKD within 90 days (eGFR <30) was a dominant predictor of long-term harm, associated with subsequent advanced CKD (SHR ~44.5) and MAKE365 (HR ~6.6), with 36% progressing to advanced CKD and 51% reaching MAKE365 by 1 year.