Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Description of hypovolemia
- Treatment and perioperative management of hypovolemia
- Management of a hypovolemic shock
Definition and mechanisms
- Also known as volume depletion or volume contraction is a state of abnormally low extracellular fluid volume
- The maintenance of an adequate fluid balance is key to preserving homeostasis
- Caused by either a loss of both sodium and water or a decrease in blood volume
- Hypovolemia refers to the loss of extracellular fluid and should not be confused with dehydration
- Untreated hypovolemia or excessive and rapid losses of volume may lead to hypovolemic shock
- Immediate treatment for hypovolemia is necessary to prevent life-threatening organ damage, shock, or death
Signs and symptoms
- Dizziness
- Headaches
- Weakness
- Thirst
- Fatigue
- Muscle cramps
- Unable to pee (urinate) or the color of the urine is darker than normal
Hypovolemic shock:
- Tachycardia
- Hypotension
- Pale or cold skin
- Cyanosis
- Confusion
- Difficulty breathing or rapid breathing
- Excessive sweating
- Oliguria
- Abdominal and chest pain
- Cold hands and feet
Stages of hypovolemic shock
| Stage 1 | Stage 2 | Stage 3 | Stage 4 | |
|---|---|---|---|---|
| Blood loss | Up to 15% (750 mL) | 15–30% (750–1500 mL) | 30–40% (1500–2000 mL) | Over 40% (over 2000 mL) |
| Blood pressure | Normal (Maintained by vasoconstriction) | Increased diastolic BP | Systolic BP < 100 | Systolic BP < 70 |
| Heart rate | Normal | Slight tachycardia (> 100 bpm) | Tachycardia (> 120 bpm) | Extreme tachycardia (> 140 bpm) with weak pulse |
| Respiratory rate | Normal | Increased (> 20) | Tachypneic (> 30) | Extreme tachypnea |
| Mental status | Normal | Slight anxiety, restless | Altered, confused | Decreased LOC, lethargy, coma |
| Skin | Pale | Pale, cool, clammy | Increased diaphoresis | Extreme diaphoresis; mottling possible |
| Capillary refill | Normal | Delayed | Delayed | Absent |
| Urine output | Normal | 20–30 mL/h | 20 mL/h | Negligible |
Causes
| Renal | Extrarenal | Anesthesia-associated relative hypovolemia |
|---|---|---|
| Diuretic excess Mineralocorticoid deficiency Ketonuria Osmotic diuresis Cerebral salt wasting syndrome Salt-wasting nephropathies | Gastrointestinal losses: vomiting and diarrhea Skin losses: excessive sweating and burns Respiratory losses: hyperventilation Build up of fluid in third spaces: - Acute pancreatitis - Intestinal obstruction - Increased vascular permeability - Hypoalbuminemia Internal bleeding Trauma | Decreased central sympathetic output Decreased cardiovascular reflex responses Decreased baroreceptor reflex activity Decreased VSM contractile response or sensitivity to neurohumoral and adrenoceptor agonists (e.g., norepinephrine) Depressed mechanisms regulating VSM cytosolic Ca2+ Reduced VSM intracellular Ca2+ concentration Reduced VSM L-type calcium channel ion transport Reduced VSM myofilament sensitivity to calcium Activation of K+ATP channels |
Complications
- Shock
- Ischemic stroke
- Myocardial infarction
- Liver failure
- Acute renal failure
- Multi-organ failure
- Death
Differential diagnosis
- Pregnancy
- Sepsis
- Hypoglycemia
- Anaphylaxis
- Anemia
- Heart failure
- Bradycardia
- Valvular pathology
Diagnosis
- Physical exam
- Central venous catheter
- Arterial line
- Blood tests: urea and electrolytes, basic metabolic panel, full blood count, glucose, blood type, and screen
- Pulse, body temperature, and blood pressure
- Kidney function tests
- Ultrasound
- Echocardiogram
Treatment
- Fluid replacement depends on the type of fluid that has been lost:
- Blood transfusion
- Fresh frozen plasma
- Other coagulation factors
- Crystalloid solution: lactated Ringer’s solution → fill both the interstitial and intravascular spaces
- Colloids (plasma substitutes): human serum albumin (5% and 25%), dextran, gelatin, hydroxyethyl starch (HES) → stay within the intravascular space
- Treating underlying illness, wounds, or burns
- Restore electrolyte balance
Perioperative management
- Minimize preoperative fasting times
- Encourage unrestricted intake of clear fluids until 2 h before elective surgery
- Asses fluid responsiveness in hemodynamically unstable adults throughout the perioperative period with passive leg raising followed by measurement of blood pressure or (ideally) stroke volume
- Administer IV fluid with an overall positive fluid balance of 1–2 L at the end of surgery
- In case of major abdominal surgery, provide an average crystalloid fluid infusion rate of 10-12 ml/kg/h during surgery and 1.5 ml/kg/h in the 24-h postoperative period
- Ensure that intravascular volume status is optimized before adding vasopressor therapy
- Measure fluid responsiveness in higher-risk patients having major surgery using an advanced hemodynamic monitor
- Apply a goal-directed hemodynamic strategy, and if needed, introduce a vasopressor or inotrope
- Aim for the early transition from IV to oral fluid therapy after surgery
- Be aware that anesthesia can also lead to relative hypovolemia
- Identify and treat relative hypovolemia
- Monitor:
- Heart rate and rhythm
- Arterial pressure/CVP
- Pulse oximetry
- End-tidal carbon dioxide
- Inhalant anesthetic concentrations
- Arterial blood gases
- Lactate
- Selection of a fluid management strategy:
-
- Minimally/moderately invasive surgery: 1-2 L of a balanced electrolyte procedure administered over a period of 30-120 minutes
- Major invasive procedures:
- Restrictive strategy: replace only fluid lost during the procedure (approximately 3 mL/kg/h) if anticipated blood loss is < 500 mL and/or without fluid shifts
- Goal-directed therapy (GDT): for procedures with an anticipated blood loss > 500 mL and/or fluid shifts use GDT with invasive dynamic hemodynamic parameters
- Avoid liberal or fixed-volume approaches that lead to the administration of large volumes of crystalloid solution, tissue edema, and associated adverse outcomes
Management of a hypovolemic shock
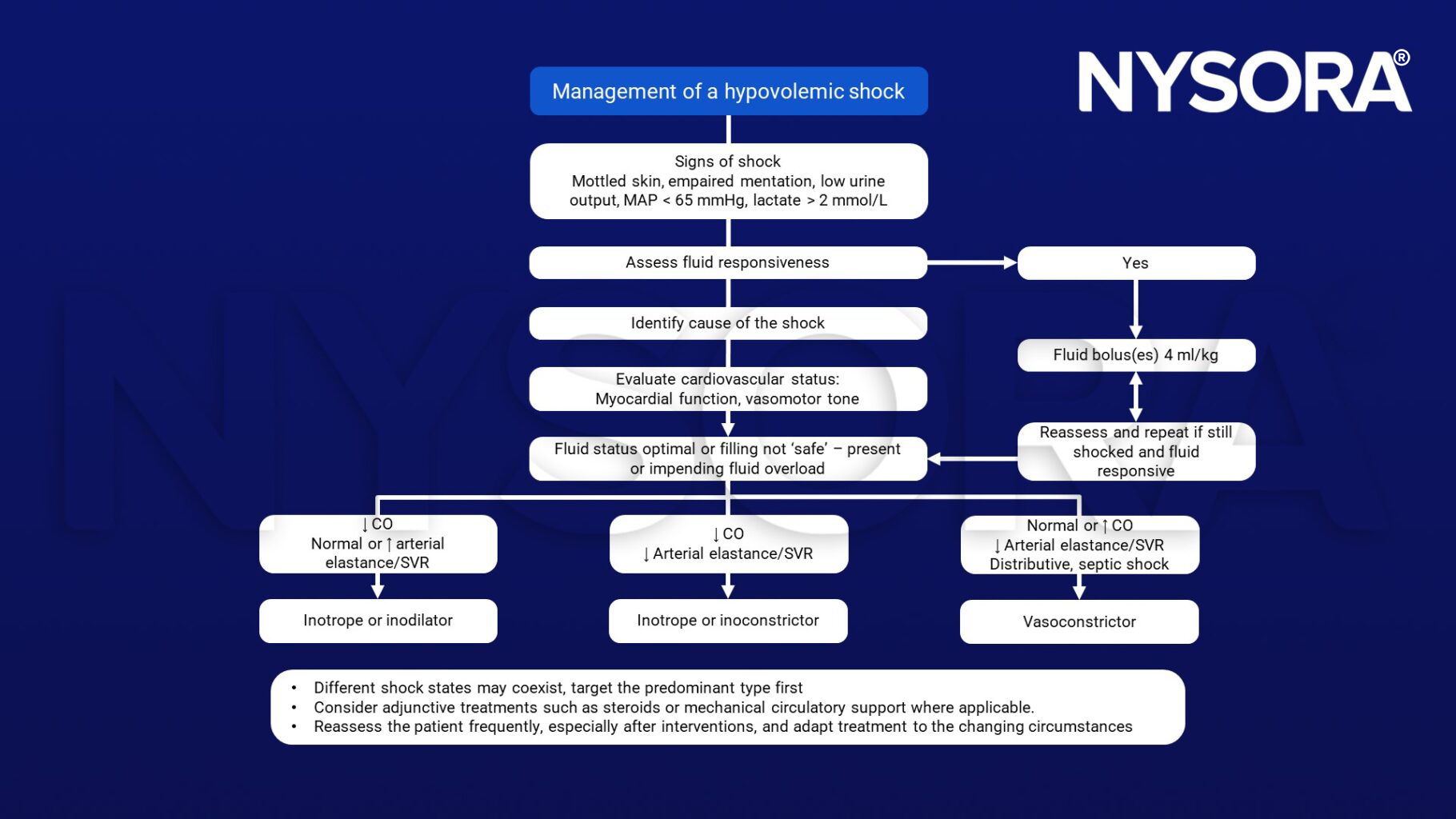
Management of a hypovolemic shock, fluid responsiveness, CO, cardiac output, arterial elastance, SVR, inotrope, inodilator, inoconstrictor, vasoconstrictor
Suggested reading
- Joshi, G. 2022. Intraoperative fluid management. Up to date. https://www.uptodate.com/contents/intraoperative-fluid-management#H254311346
- Jha, A., Zilahi, G., Rhodes, A., 2021. Vasoactive therapy in shock. BJA Education 21, 270–277.
- Timothy E. Miller, Paul S. Myles; Perioperative Fluid Therapy for Major Surgery. Anesthesiology 2019; 130:825–832.
- Noel-Morgan J, Muir WW. Anesthesia-Associated Relative Hypovolemia: Mechanisms, Monitoring, and Treatment Considerations. Front Vet Sci. 2018;5:53.
- Al-Khafaji, A., Webb, A. 2004. Fluid resuscitation. Continuing Education in Anaesthesia Critical Care & Pain. 4;4:127-131.
Clinical updates
Markl-Le Levé et al. (Current Opinion in Anesthesiology, 2025) refine the modern understanding of hypovolemia by emphasizing that treatment should prioritize physiology-guided volume restoration rather than liberal fluid replacement. Their review highlights how excessive crystalloids can worsen dilutional coagulopathy, tissue edema, and organ dysfunction, reinforcing perioperative strategies that assess fluid responsiveness, correct the underlying cause of volume loss, and integrate early hemostatic therapy when hypovolemia progresses to shock.
- Read more about this study HERE.