Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Recognize signs and symptoms of alcohol withdrawal syndrome and delirium tremens
- Manage and treat alcohol withdrawal syndrome and delirium tremens
Definition and mechanism
- Alcohol withdrawal syndrome (AWS) is a set of symptoms that occur following a reduction in alcohol use after a period of excessive use
- Symptoms can be suppressed by alcohol intake and are more common in the postoperative period
- AWS starts typically after 6-24 hours without alcohol and is most pronounced at 24-36 hours, however, can be delayed for up to 5 days
- AWS results from neurological changes after long-term alcohol use:
- Ethanol binds to postsynaptic GABAA receptors, thereby enhancing their inhibitory effect
- The resulting chronic excitatory suppression leads to an increased brain synthesis of excitatory neurotransmitters such as norepinephrine, 5-hydroxytryptamine, and dopamine
- The brain is flooded with increased levels of excitatory neurotransmitters when the inhibitory effects of ethanol are withdrawn
- Delirium tremens is a rapid onset of confusion due to alcohol withdrawal
- Delirium tremens occurs in 5% of patients experiencing withdrawal
- Mortality rate of delirium tremens is 10% (due to hypotension, dysrhythmias or seizures)
Signs and symptoms
| AWS | Delirium tremens |
|---|---|
| Tremors Nightmares Hallucinations Gastric upset Nausea Vomiting Hyperreflexia Anxiety Agitation Mild confusion Insomnia Autonomic nervous system hyperactivity (tachycardia, Hypertension, cardiac dysrhythmia) | Shaking Shivering Tachycardia Sweating Hallucinations Hyperthermia Nausea Vomiting Seizures Agitation Aggression Tachycardia Hypertension or Hypotension Grand mal seizures |
Medical disorders associated with alcoholism
| CNS | Wernicke–Korsakoff syndrome Peripheral neuropathy Autonomic dysfunction |
| CVS | Cardiomyopathy Heart failure Hypertension Arrhythmias (e.g. AF, SVT, VT) |
| GI | Alcoholic liver disease Pancreatitis Gastritis Oesophageal and bowel carcinoma |
| Metabolic | Hyperlipidemia Obesity Hypoglycemia Hypokalemia Hypomagnesemia Hyperuricemia |
| Hematological | Macrocytosis Thrombocytopenia Leucopenia |
| Musculoskeletal | Myopathy Osteoporosis Osteomalacia |
Treatment
Prophylactic treatment before the onset of AWS symptoms
- Benzodiazepines or clomethiazole
- Oral or enterally applied alcohol administration (0.5 g/kg body weight/day)
- Adjuncts such as alpha2-agonists
Benzodiazepines are the first-line treatment for AWS and delirium tremens
Class Example Duration of action Route of administration Dose
Benzodiazepines Chlordiazepoxide Long p.o.
Prophylaxis: 5-25 mg
Treatment: 50 -100 mg
Lorazepam Short p.o./IV
Prophylaxis: 0.5-2 mg
Treatment: 1-8 mg
Other agents
Diazepam Long p.o./IV
Prophylaxis: 2.5-10 mg
Treatment: 10-40 mg
Clomethiazole p.o.
Prophylaxis: 9-12 capsules in 24h
Haloperidol p.o./IV/IM
Treatment: 0.5-20 mg
Clonidine IV Treatment: 0.1-1 mg bolus/0.1-4 µg/kg/h
- Be aware that the required doses for severe AWS can vary substantially within the first 24h
- Clomethiazole is not advised in critically ill patients due to bronchial secretion and a elevated risk of pneumonia
- Non-benzodiazepine agents should be used in conjunction with benzodiazepines
- Beta-adrenergic blockers and centrally acting alpha-adrenergic agonists (clonidine, dexmedetomidine) achieve symptomatic control but they do not reduce the incidence of delirium or seizures
- Haloperidol (for severe agitation or hallucinations) may increase the risk of seizures
- Consider anticonvulsant agents such as carbamazepine, sodium valproate, and topiramate
General treatment
- Correct metabolic (potassium, magnesium, and thiamine) and hemodynamic derangements
- Correct fluid and blood product deficits
- General supportive care (early nutrition)
- Severe cases will need ICU admission & propofol infusion/dexmedetomidine & possible intubation
- Offer psychosocial support: counseling and detoxification/rehab
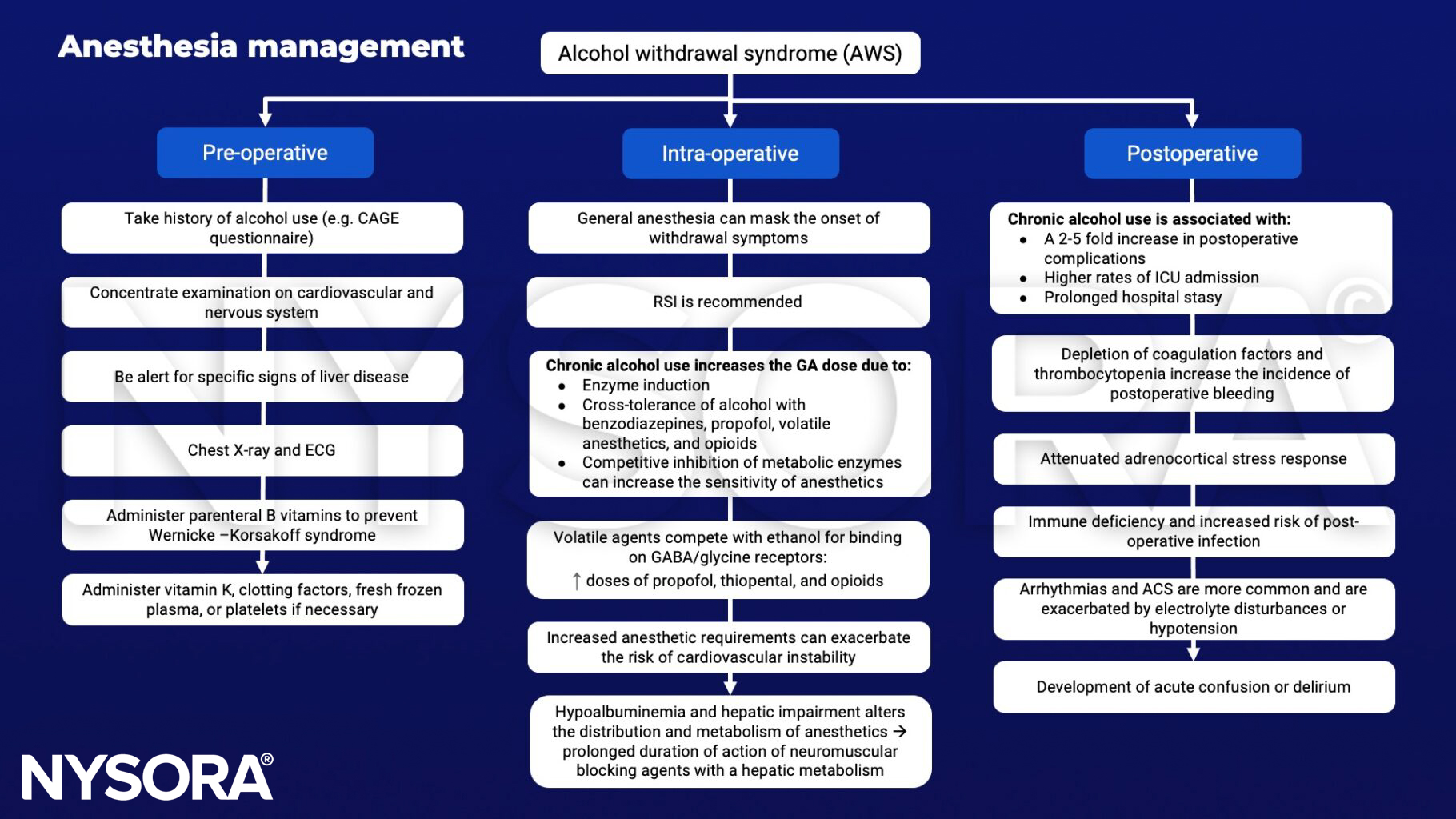
Management
Keep in mind
As the severity of withdrawal symptoms can vary greatly, a scale such as the CIWA-Ar is useful for:
- Monitoring the effectiveness of prophylactic treatment or fixed-schedule treatment regimens
- Guiding administration in symptom-triggered treatment regimens
Suggested reading
- Ungur A, L, Neumann T, Borchers F, Spies C: Perioperative Management of Alcohol Withdrawal Syndrome. Visc Med 2020;36:160-166.
- Chapman, Richard & Plaat, Felicity. (2009). Alcohol and anaesthesia. Continuing Education in Anaesthesia, Critical Care & Pain. 9. 10-13.
Clinical updates
Lane et al. (RAPM, 2024) emphasize that alcohol withdrawal syndrome (AWS) is common and often underrecognized in the perioperative period, with postoperative stress, fasting, and abrupt alcohol cessation increasing the risk of severe withdrawal and delirium tremens. The review reinforces early screening for alcohol use disorder, proactive prophylaxis with benzodiazepines, and prompt correction of metabolic derangements (especially magnesium, potassium, and thiamine) as key strategies to prevent seizures, delirium, and cardiovascular instability.
- Read more about this study HERE.
Piland et al. (Anesthesia & Analgesia, 2025) report that alcohol use disorder contributes to 10–20% of ICU admissions, with alcohol withdrawal syndrome (AWS) being a major driver of prolonged ICU stay and mechanical ventilation. Early screening and proactive management are essential. Symptom-triggered benzodiazepines remain first-line therapy, with dexmedetomidine or ketamine considered in refractory cases. Structured protocols, thiamine supplementation, and multidisciplinary involvement improve outcomes.
- Read more about this study HERE.