Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About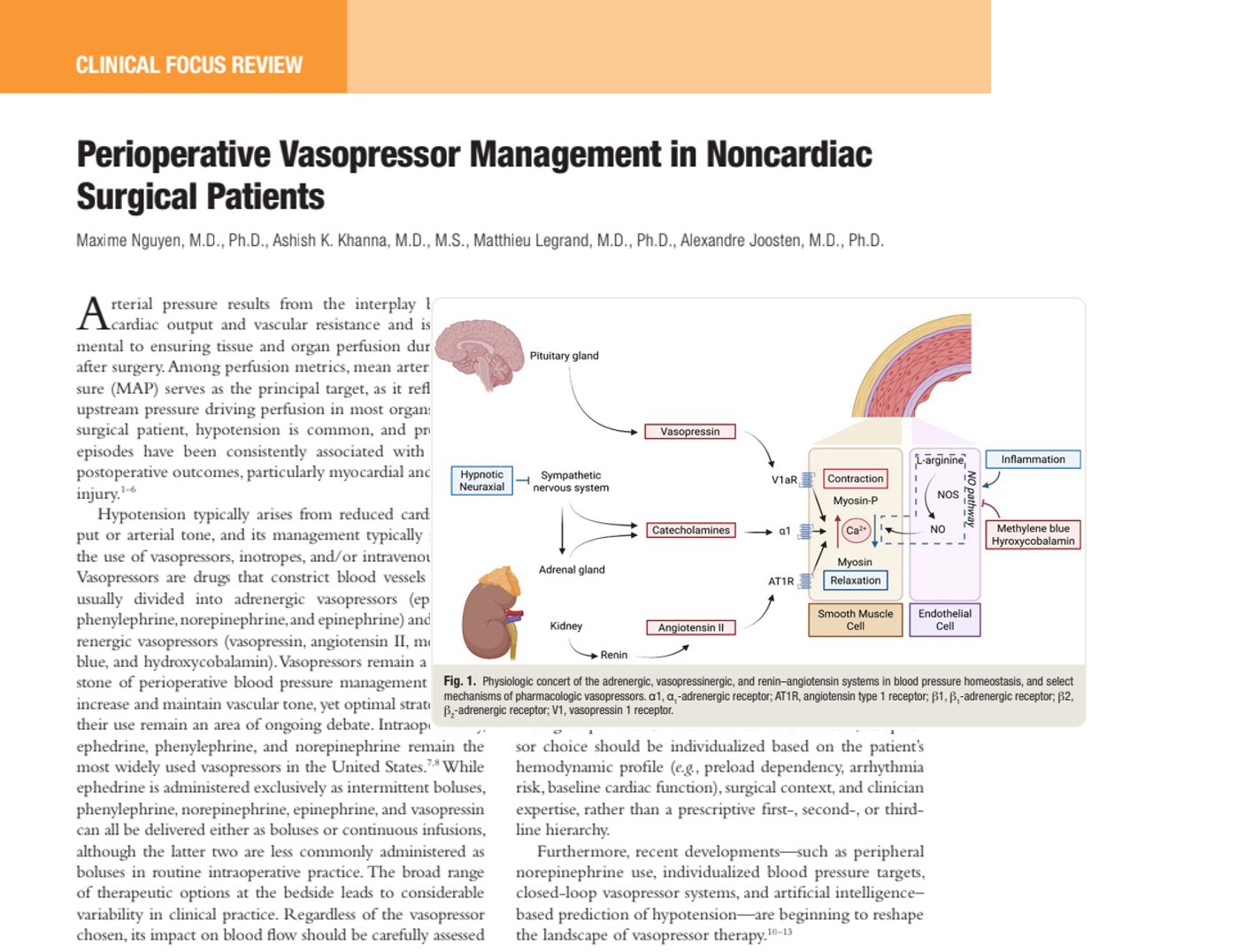

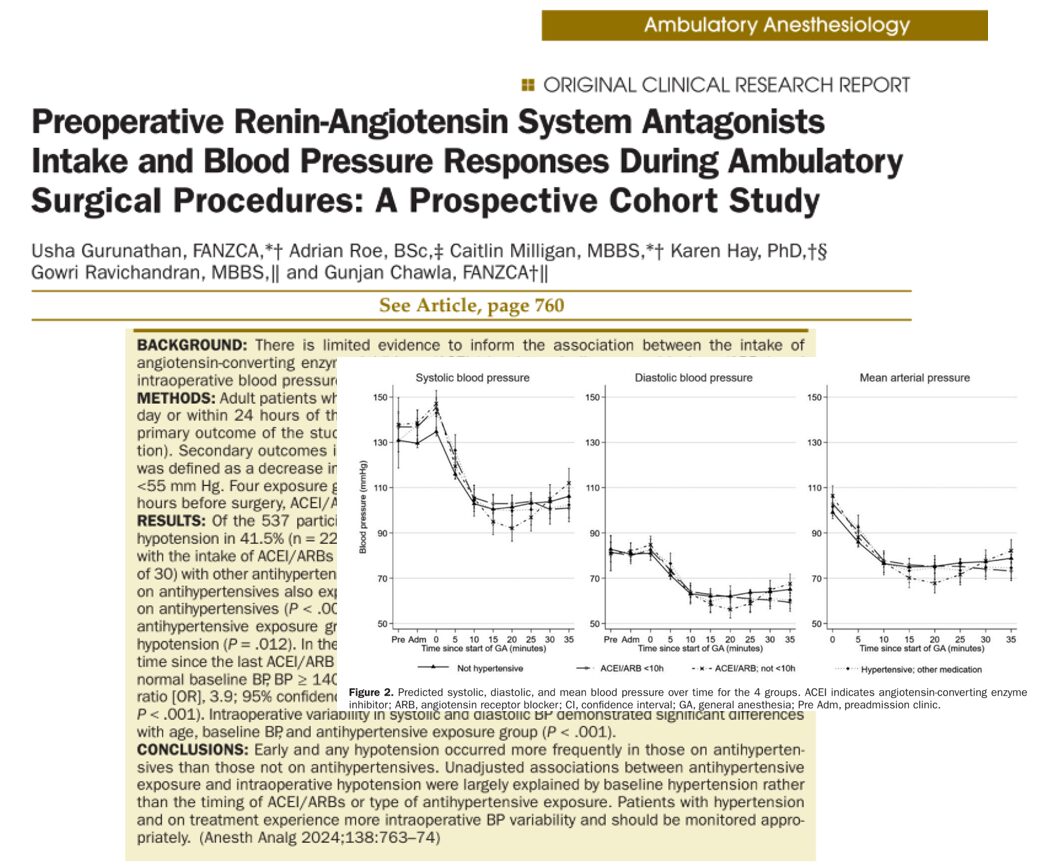
Perioperative hypotension remains one of the most critical challenges in modern anesthesia and surgical care. Maintaining adequate mean arterial pressure (MAP) is essential to ensure sufficient tissue perfusion and prevent postoperative complications such as acute kidney injury (AKI) and myocardial injury.
A recent clinical review highlights the expanding role of vasopressors, emerging technologies, and individualized strategies in optimizing hemodynamic stability during noncardiac surgery.
Understanding arterial pressure and perfusion
Arterial pressure is determined by the interaction between:
- Cardiac output (CO)
- Systemic vascular resistance (SVR)
MAP is widely used as the primary clinical target because it reflects the driving pressure for organ perfusion.
Why hypotension matters
Even short periods of intraoperative hypotension can lead to:
- Myocardial ischemia
- Acute kidney injury
- Increased postoperative morbidity
Mechanisms of hypotension in surgical patients
1. Vasodilation (most common cause)
Vascular tone is regulated by:
- Sympathetic nervous system
- Vasopressin system
- Renin–angiotensin–aldosterone system
During surgery:
- Anesthetic agents suppress sympathetic tone
- Nitric oxide (NO) increases vasodilation
- Inflammatory mediators worsen vascular relaxation
2. Reduced cardiac output
Caused by:
- Hypovolemia
- Cardiac dysfunction
- Increased venous capacitance
What are vasopressors?
Vasopressors are pharmacologic agents that:
- Increase vascular tone
- Elevate blood pressure
- Improve organ perfusion
They are broadly classified into:
Adrenergic vasopressors
- Norepinephrine
- Phenylephrine
- Ephedrine
- Epinephrine
Non-adrenergic vasopressors
- Vasopressin
- Angiotensin II
- Methylene blue
- Hydroxocobalamin
Mechanism of action: how vasopressors work
Vasopressors influence circulation:
- α1 receptor stimulation → vasoconstriction
- β1 receptor stimulation → increased heart rate and contractility
- V1a receptor activation (vasopressin) → direct vasoconstriction
Common vasopressors used in the operating room
Norepinephrine
- Mixed α1 and β1 agonist
- First-line in many shock states
- Provides stable blood pressure control
Phenylephrine
- Pure α1 agonist
- May reduce cardiac output
- Useful in patients with arrhythmias
Ephedrine
- Indirect and direct adrenergic effects
- Preserves cardiac output
- Risk of tachyphylaxis with repeated use
Comparison of vasopressors
Hemodynamic effects:
- Phenylephrine → ↑ SVR, ↓ or neutral CO
- Norepinephrine → ↑ SVR with preserved CO
- Ephedrine → ↑ CO and heart rate
- Vasopressin → ↑ SVR without cardiac stimulation
Step-by-step approach to hypotension management
Step 1: Identify the cause
Assess:
- Blood loss
- Anesthetic depth
- Cardiac function
- Infection or inflammation
Step 2: Evaluate hemodynamic signals
- Low diastolic pressure → suggests vasodilation
- Narrow pulse pressure → suggests low stroke volume
Step 3: Decide between fluids or vasopressors
Use clinical indicators:
- Hypovolemia → fluids first
- Vasodilation → vasopressors
Step 4: Initiate therapy
- Start with a first-line vasopressor
- Titrate based on MAP response
Step 5: Reassess continuously
- Monitor perfusion
- Adjust therapy dynamically
Fluids vs vasopressors: which comes first?
Use fluids when:
- Evidence of hypovolemia
- Low stroke volume
- Positive fluid responsiveness tests
Use vasopressors when:
- Low arterial tone
- Normal or high cardiac output
- Anesthesia-induced vasodilation
Key insight: Fluids and vasopressors are complementary, not competing therapies.
Second-line therapies and adjuncts
Vasopressin
- Used when norepinephrine is insufficient
- May reduce the need for catecholamines
Angiotensin II
- Effective in refractory vasodilatory shock
- Potential renal benefits
Methylene blue
- Inhibits the nitric oxide pathway
- Limited evidence, potential risks
Hydroxocobalamin
- Scavenges nitric oxide
- Associated with kidney injury
Risks and complications of vasopressors
Potential adverse effects include:
- Excessive vasoconstriction → tissue ischemia
- Arrhythmias (β1 stimulation)
- Increased myocardial oxygen demand
- Organ hypoperfusion
Advances in vasopressor therapy
1. Peripheral norepinephrine use
- Now considered safe at low doses
- Enables rapid initiation of therapy
2. Individualized blood pressure targets
- Tailored to patient physiology
- Based on autoregulation thresholds
3. Artificial intelligence and prediction tools
- Machine learning models can predict hypotension
- Early intervention may improve outcomes
4. Closed-loop vasopressor systems
Automated systems can:
- Adjust infusion rates in real-time
- Reduce hypotensive episodes
- Improve time within the target MAP
Clinical pearls
- Avoid prolonged hypotension at all costs
- Choose vasopressors based on physiology, not habit
- Monitor both pressure and perfusion
- Reassess frequently
- Use multimodal strategies
Conclusion
Perioperative vasopressor management is rapidly evolving. While traditional pharmacologic principles remain foundational, emerging innovations, including closed-loop systems, AI-guided prediction, and individualized hemodynamic targets, are transforming clinical practice.
Ultimately, optimal outcomes depend on:
- Understanding the underlying physiology
- Tailoring therapy to the individual patient
- Integrating new technologies with clinical judgment
As ongoing trials such as VEGA-2 continue to provide evidence, the future of perioperative hemodynamic management is poised to become increasingly precise, personalized, and data-driven.
Reference: Nguyen M et al. Perioperative Vasopressor Management in Noncardiac Surgical Patients. Anesthesiology. 2026;144:670-682.
Download the Anesthesia Assistant App HERE for step-by-step educational support. Describe your case and get a structured answer.