Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About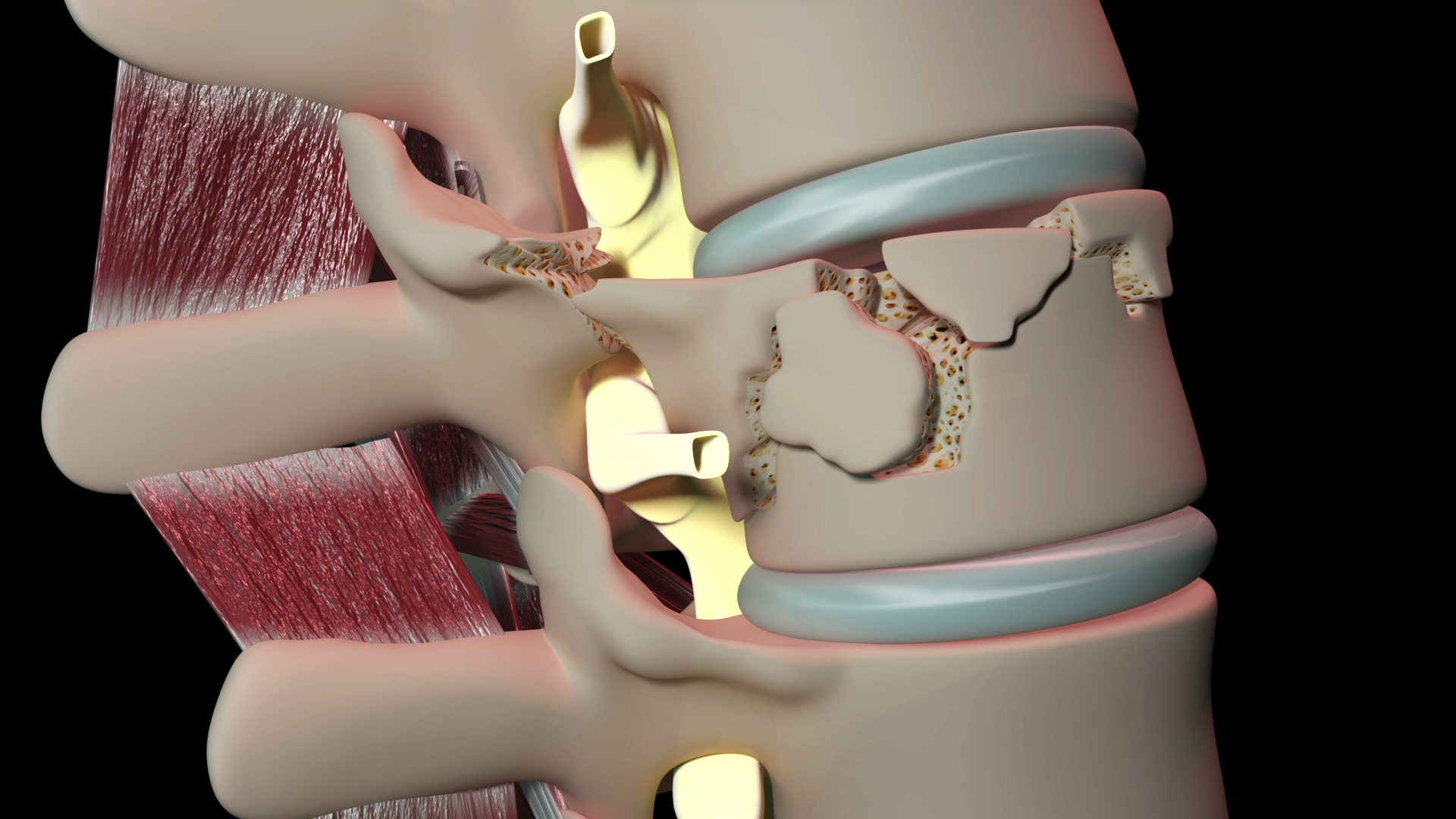
Learning objectives
- Describe the mechanisms of and recognize acute spinal cord injury
- Classify spinal cord injury
- Manage patients with acute spinal cord injury
Definition & mechanisms
- Spinal cord injury (SCI) consists of damage to the spinal cord caused by an insult resulting in the transient or permanent loss of spinal motor, sensory, and autonomic function
- Approximately 14% of vertebral column fractures result in damage to the spinal cord
Signs
- Diaphragmatic breathing
- Hypotension without an obvious cause
- Bradycardia
- Priapism
- Flaccid areflexia
- Loss of pain response below a level
Pathophysiology
- Primary injury
- Results from direct cord compression, hemorrhage, and traction forces
- Mechanisms:
- Subluxation of the vertebral elements causes a pincer-like direct damage to the cord
- Hyperextension can cause compression of the cord between the ligamentum flavum and anterior osteophytes
- Retropulsion of bone or disc fragments can cause either damage to the cord via direct cord compression or via impairment to the vascular supply
- Penetrating injury can also cause direct compression and vascular injury
- Secondary injury
- Within minutes after injury, secondary damage starts developing
- Hemorrhage in the central grey matter damages neuronal cell membranes
- Spinal cord edema and subsequent spinal cord ischemia
- Ischemia extends bidirectionally, along the site of injury within hours
- Systemic effects, local vasomotor changes, the release of free radicals, intracellular electrolyte shifts, neurotransmitters, cord edema, disruption of cell metabolism, and cell death are all thought to be involved in secondary injury
- Prevention of secondary injury may make a dramatic difference to the quality of life of patients
- Neurogenic shock
- Interruption of autonomic pathways leading to hypotension, bradycardia, and hypothermia
- Spinal shock
- Loss of reflexes below the level of SCI
- Gradual return of reflex activity when the reflex arcs below redevelop, often resulting in spasticity and autonomic hyperreflexia
Classification
American Spinal Injury (ASIA) impairment scale:
| A: Complete | No motor or sensory function is preserved in the sacral segments S4-5 |
| B: Sensory incomplete | Sensory but not motor function is preserved below the neurologic level & includes the sacral segments |
| C: Motor incomplete | Motor function is preserved below the neurologic level & more than half of key muscle functions below the neurologic level of injury have a muscle grade <3 |
| D: Motor incomplete | Motor function is preserved below the neurologic level & at least half (half or more) of key muscle functions below the neurologic level of injury have a muscle grade ≥3 |
| E: Normal | Sensation & motor function are graded as normal in all segments |
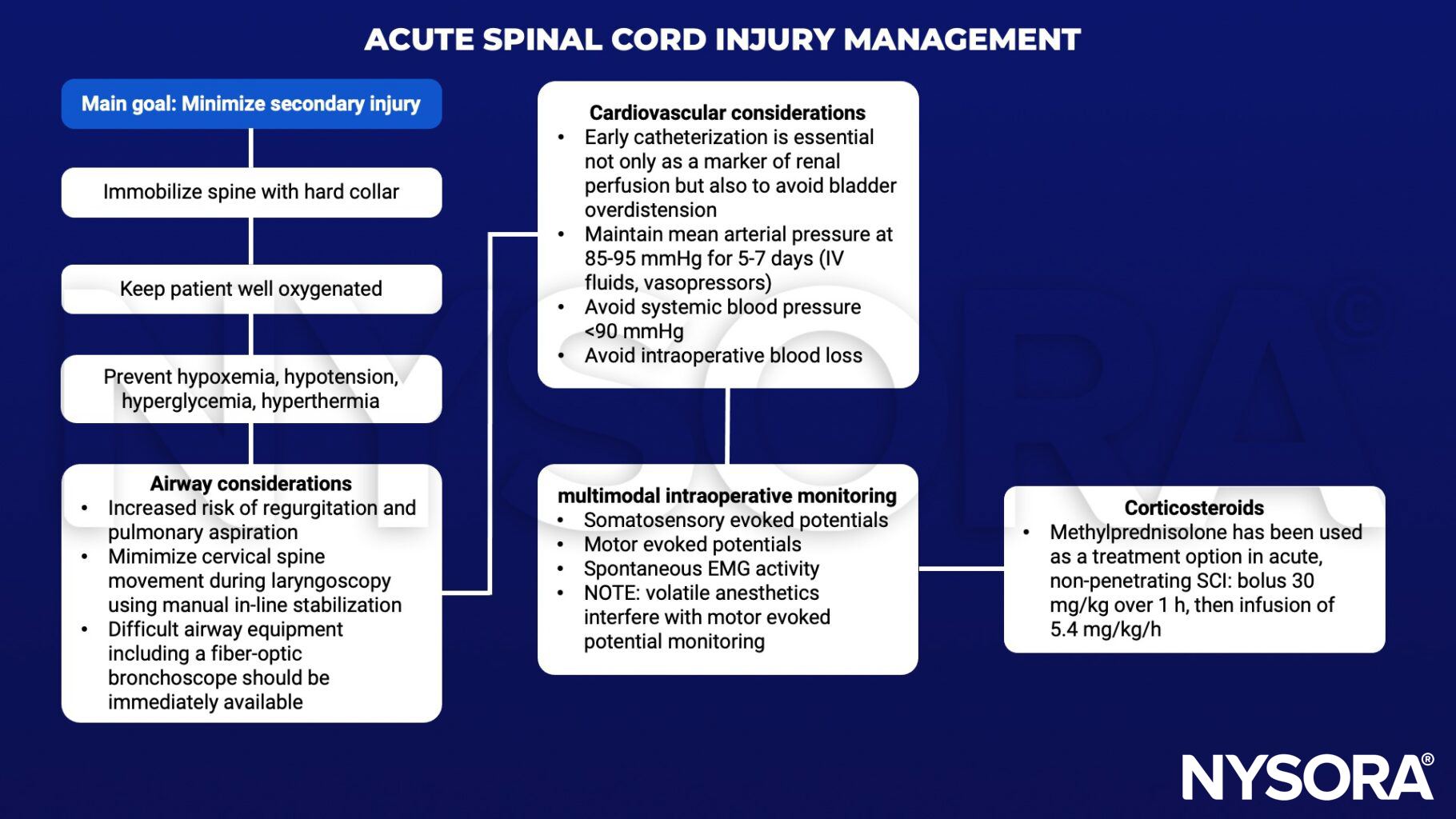
Management
Suggested reading
- Bonner S, Smith C. Initial management of acute spinal cord injury. Continuing Education in Anaesthesia Critical Care & Pain. 2013;13(6):224-31.
- Dooney N, Dagal A. Anesthetic considerations in acute spinal cord trauma. Int J Crit Illn Inj Sci. 2011;1(1):36-43.