Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe Marfan’s syndrome
- Recognize signs and symptoms of Marfan’s syndrome
- Anesthetic management of a patient with Marfan’s syndrome
Definition and mechanisms
- Marfan’s syndrome (MFS) is an autosomal dominant condition of connective tissue, mainly involving the cardiovascular, musculoskeletal, and ocular systems
- MFS is caused by a mutation in the FBN1 gene on chromosome 15 that encodes the protein fibrillin
- The connective tissue abnormalities lead to connective tissue weakness with hyperextensible joints, eyes (dislocation of the lens), increased risk of valvular/aortic dissection, and spontaneous pneumothorax
Signs and symptoms
- Ocular: Lens dislocation, myopia, retinal detachment, glaucoma
- Cardiovascular: Aortic root dilatation with aortic regurgitation, aneurysm formation, aortic dissection, mitral valve prolapse with mitral regurgitation
- Musculoskeletal: Long bone overgrowth, scoliosis, kyphosis, joint hypermobility, pectus carinatum/excavatum, high-arched palate
- Respiratory: Spontaneous pneumothorax
- Skin: Striae
- Central nervous system: Dural ectasia
Complications
- Patients with MFS and left ventricular dilatation are at risk of ventricular arrhythmias
- Aortic root diameter >4 cm carries a risk of aortic dissection
Treatment
- Medications
- β-blockers
- Calcium channel blockers or ACE inhibitors if β-blockers are contraindicated/not tolerated
- Surgery to repair the aorta or replace a heart valve
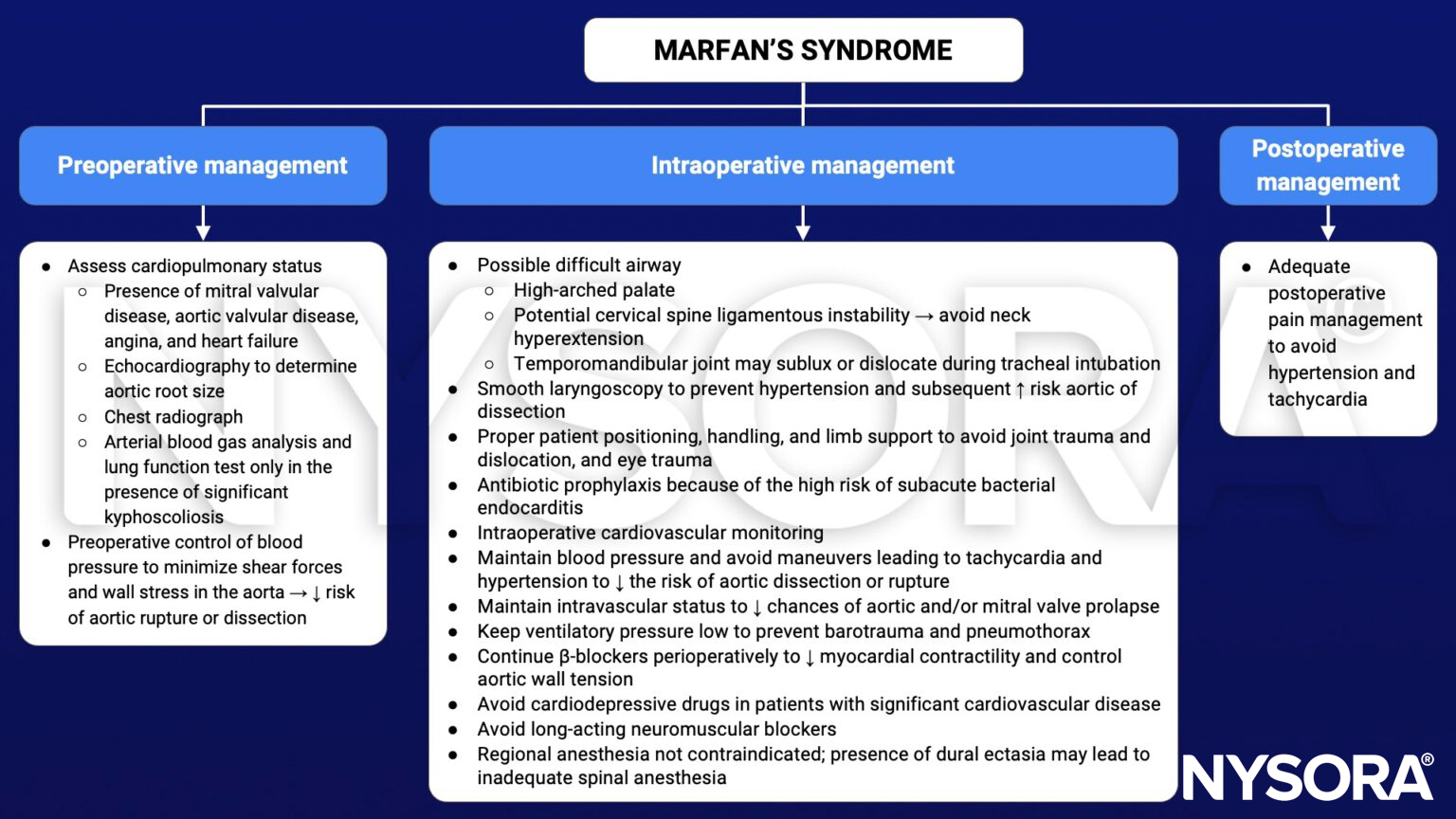
Management
Obstetric anesthesia
- If no symptoms and aorta diameter <4 cm: No special considerations and vaginal delivery ok
- If aortic root dilation and aortic regurgitation: Multidisciplinary management with cardiology/cardiac surgery/obstetrics
- Some recommend caesarean section if aorta diameter >4.5 cm and labor if aorta diameter >4 and <4.5 cm
- Problems
- Airway might be even more difficult
- Neuraxial anesthesia for vaginal delivery and caesarean section
- Aortic dilatation with risk of dissection or rupture
- Perform monthly echocardiography during pregnancy
- Reduce shear forces on aorta
- Consider very early epidural placement
- Need for invasive monitoring
- Drug therapy to prevent hypertension and tachycardia (e.g., labetalol)
- Dural ectasia
- Higher risk for failed epidural, dural puncture, and postdural puncture headache
- Consider CT/MRI
Keep in mind
- Prevent a sudden increase in myocardial contractility, producing an increase in aortic wall tension, which could lead to aortic dissection
- Preexisting cardiovascular disease and the potential for acute cardiovascular and respiratory complications in patients with MFS require careful preoperative assessment and the use of a skillful anesthetic technique to avoid fatal complications
- Blood pressure control is the central component of perioperative management
Suggested reading
- Araújo MR, Marques C, Freitas S, Santa-Bárbara R, Alves J, Xavier C. Marfan Syndrome: new diagnostic criteria, same anesthesia care? Case report and review. Braz J Anesthesiol. 2016;66(4):408-413.
- Castellano JM, Silvay G, Castillo JG. Marfan Syndrome: Clinical, Surgical, and Anesthetic Considerations. Seminars in Cardiothoracic and Vascular Anesthesia. 2014;18(3):260-271.
- Allyn J, Guglielminotti J, Omnes S, Guezouli L, Egan M, Jondeau G, Longrois D, Montravers P. Marfan’s Syndrome During Pregnancy: Anesthetic Management of Delivery in 16 Consecutive Patients. Anesthesia & Analgesia. 2013;116(2): 392-398.
- Marfan Syndrome. In: Bissonnette B, Luginbuehl I, Marciniak B, Dalens BJ. eds. Syndromes: Rapid Recognition and Perioperative Implications. McGraw Hill; 2006. Accessed January 26, 2023.