Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About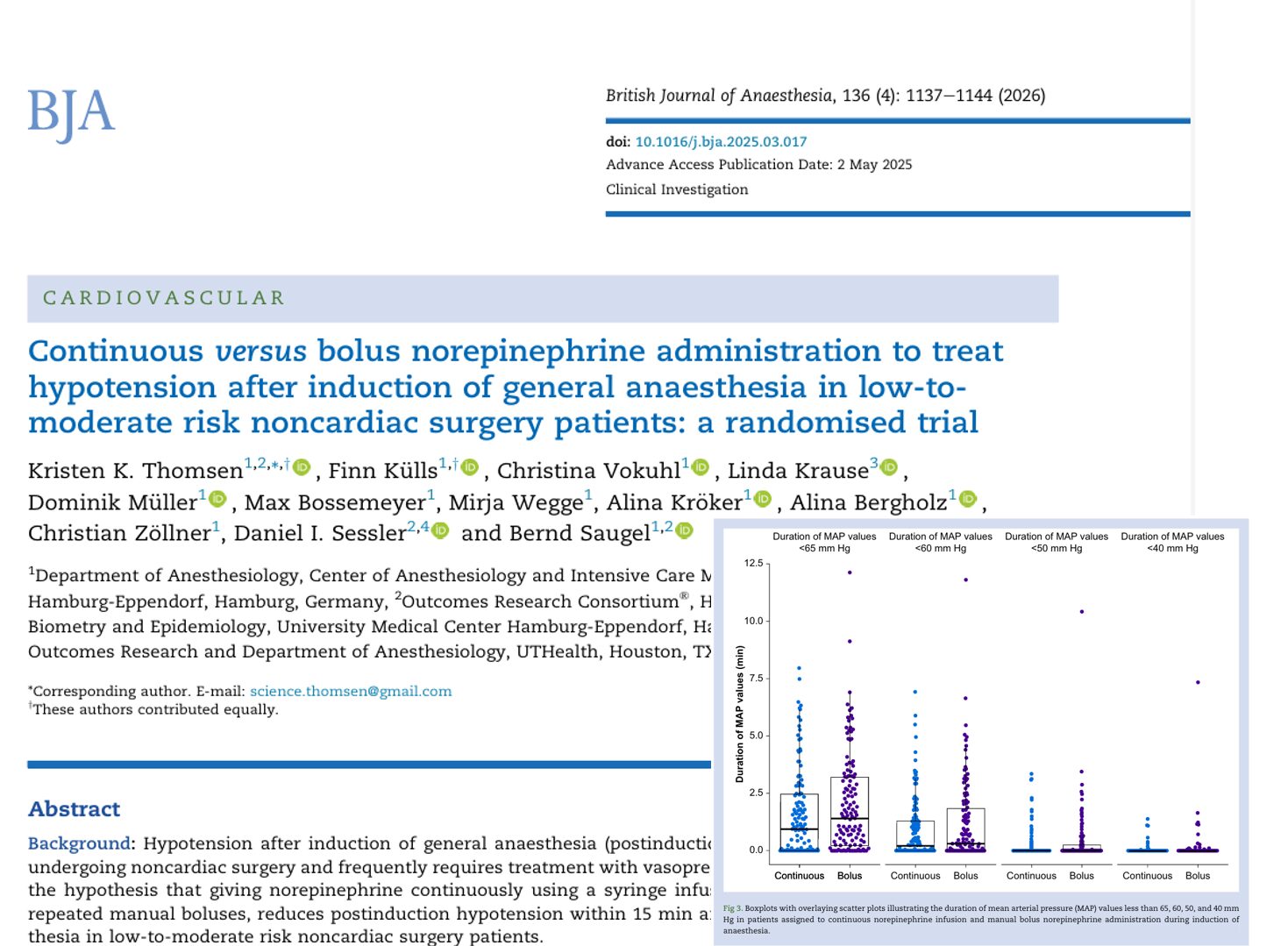

Introduction
A newly published randomized clinical trial in the British Journal of Anaesthesia (2026) evaluates whether continuous norepinephrine infusion offers superior hemodynamic stability compared to intermittent bolus dosing during the induction of general anesthesia.
Postinduction hypotension remains a frequent and clinically significant complication in noncardiac surgery. It is strongly associated with adverse outcomes, including:
- Acute kidney injury
- Myocardial injury
- Increased perioperative morbidity
Maintaining mean arterial pressure (MAP) above 60–65 mm Hg is widely recommended to prevent organ hypoperfusion.
This study provides important insights into optimizing vasopressor administration strategies during anesthesia induction.
What is postinduction hypotension?
Postinduction hypotension refers to a drop in arterial blood pressure occurring shortly after induction of general anesthesia.
Key mechanisms
- Vasodilation caused by anesthetic agents (e.g., propofol)
- Reduced sympathetic tone
- Decreased cardiac output
Clinical importance
- Occurs in up to one-third of patients before surgical incision
- Even brief episodes can contribute to organ injury
- Severity and duration both influence risk
Study overview
Design and population
- Type: randomized controlled trial (INDUCT trial)
- Participants: 276 patients (261 analyzed)
- Age: median 62 years
- Risk profile: low-to-moderate risk, noncardiac surgery
- Setting: University Medical Center Hamburg-Eppendorf
Intervention groups
- Continuous infusion group
- Norepinephrine via syringe infusion pump
- Dose range: 0.03–0.2 µg/kg/min
- Bolus group
- Intermittent manual IV boluses
- Typical doses: 5–20 µg
Monitoring
- Intermittent oscillometric blood pressure (every 2.5 minutes)
- Blinded continuous finger-cuff monitoring for data analysis
Primary outcome explained
The primary endpoint was: Area under MAP < 65 mm Hg within 15 minutes after induction
This metric integrates:
- Depth of hypotension
- Duration of hypotension
How it works
- Measure MAP continuously
- Identify values below 65 mm Hg
- Calculate the difference from the threshold
- Multiply by the time duration
- Sum all values
Key findings
Primary outcome
- Continuous infusion: 3.6 mm Hg·min
- Bolus administration: 5.5 mm Hg·min
- Result: No statistically significant difference (P = 0.070)
Interpretation
Although numerically lower in the infusion group, the difference was:
- Not statistically significant
- Not clinically meaningful
Secondary outcomes
Incidence of hypotension (MAP <65 mm Hg)
- Continuous: 69% of patients
- Bolus: 82% of patients
Suggests slightly fewer hypotensive episodes with infusion
Duration of hypotension
- Continuous: 1.0 minute
- Bolus: 1.4 minutes
Minimal difference
Severe hypotension (MAP <40 mm Hg)
- Continuous: 8%
- Bolus: 15%
This finding raises the possibility that continuous infusion may reduce extreme hypotensive episodes, which are thought to contribute disproportionately to organ injury.
Norepinephrine dosing differences
Total drug exposure
- Continuous infusion: 0.9 µg/kg
- Bolus dosing: 0.3 µg/kg
Patients receiving continuous infusion were exposed to approximately three times more norepinephrine.
Clinical implications
- Continuous infusion provides steady hemodynamic support
- Bolus dosing results in peaks and troughs in blood pressure
- Higher drug exposure did not translate into better outcomes
Risk of hypertension
A key concern with continuous vasopressor infusion is overtreatment, leading to hypertension.
Study findings
There were no significant differences between groups in:
- MAP > 100 mm Hg
- MAP > 110 mm Hg
- MAP > 120 mm Hg
Continuous infusion did not increase the risk of hypertension.
This is clinically reassuring, as intraoperative hypertension is generally less harmful than hypotension but still undesirable.
Clinical implications
What should clinicians do?
This study suggests that both strategies are acceptable for managing blood pressure during anesthesia induction.
When to consider continuous infusion
- High variability in patient hemodynamics
- Need for tight blood pressure control
- Availability of infusion pumps and monitoring
When to consider bolus dosing
- Rapid correction of sudden hypotension
- Simpler workflow in resource-limited settings
- Experienced clinicians comfortable with titration
Conclusion
The INDUCT trial provides robust evidence that continuous norepinephrine infusion does not significantly reduce postinduction hypotension compared to intermittent bolus dosing in low-to-moderate risk noncardiac surgery patients.
Reference: Thomsen KK et al. Continuous versus bolus norepinephrine administration to treat hypotension after induction of general anaesthesia in low-to-moderate risk noncardiac surgery patients: a randomised trial. Br J Anaesth. 2026;136:1137-1144.
Compare infusion vs bolus norepinephrine → explore the physiology and principles in the NYSORA Anesthesia Assistant app.