Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About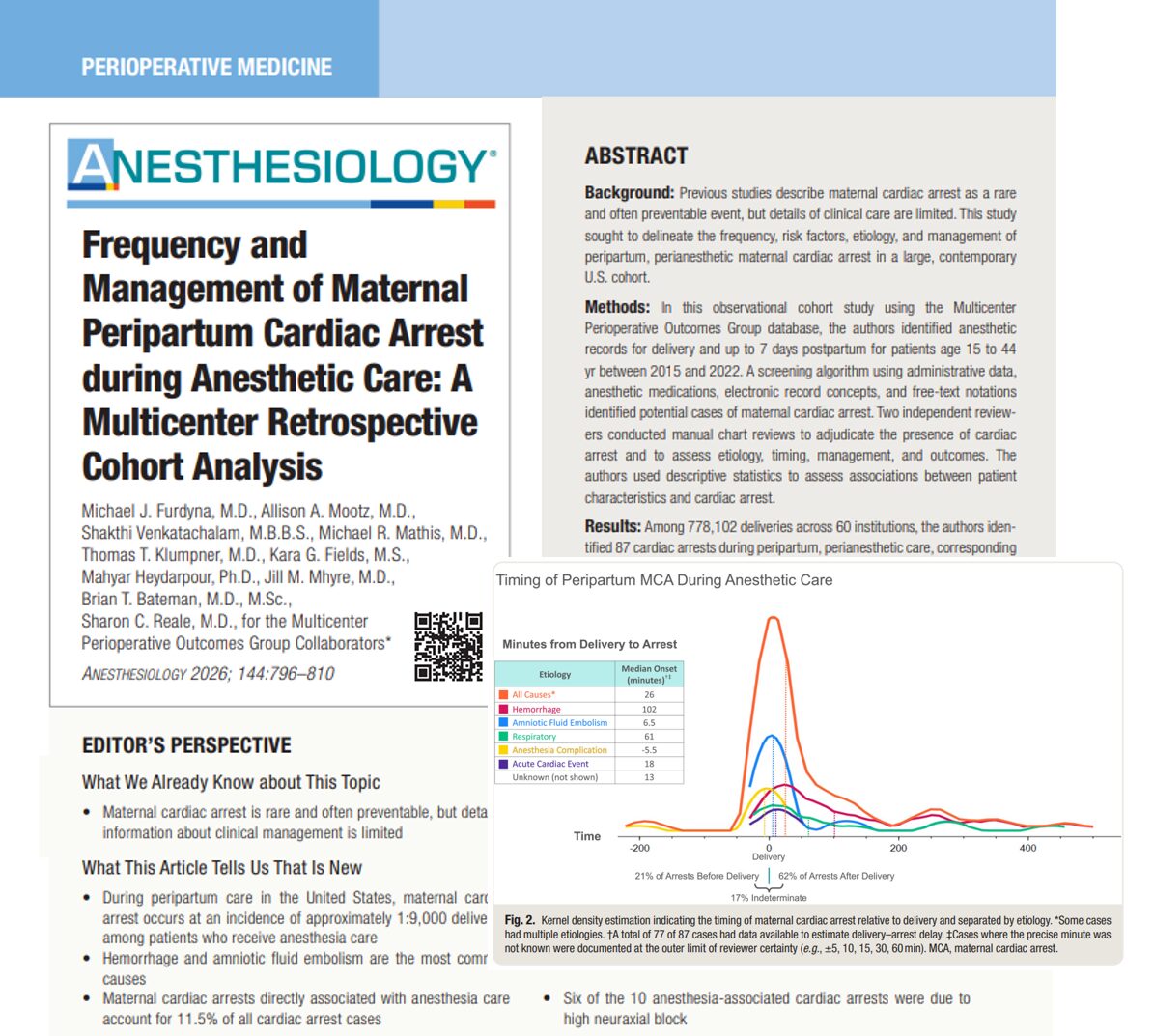





Maternal cardiac arrest (MCA) during the peripartum period remains one of the most critical emergencies in obstetric medicine. A newly published multicenter cohort study in Anesthesiology (2026) provides one of the most comprehensive analyses to date, offering detailed insights into incidence, etiology, risk factors, and management during anesthetic care.
Overview of the study
This large retrospective cohort study analyzed 778,102 deliveries across 60 U.S. institutions between 2015 and 2022. The investigation focused specifically on cardiac arrest occurring during or within 7 days of anesthetic care.
Key findings
- Incidence:
- 11.2 per 100,000 deliveries (~1 in 9,000)
- Total cases identified:
- 87 confirmed maternal cardiac arrests
- Survival outcomes:
- Return of spontaneous circulation (ROSC): 77%
- 30-day survival: 67.8%
- Primary causes:
- Hemorrhage: 40.2%
- Amniotic fluid embolism (AFE): 31.0%
- Anesthesia-related arrests:
- 11.5% of cases
What is maternal cardiac arrest?
Maternal cardiac arrest refers to the cessation of effective cardiac output during pregnancy or postpartum, resulting in loss of perfusion to vital organs.
Clinical definition
- Absence of pulse or cardiac activity
- Requires Advanced Cardiac Life Support (ACLS) interventions
- Occurs during pregnancy or within 42 days postpartum (in broader definitions)
Incidence and timing
When do cardiac arrests occur?
The study revealed important timing patterns:
- 62.1% occurred after delivery
- 20.7% occurred before delivery
- 85% occurred within 12 hours postpartum
- Median onset: 26 minutes after delivery
Location of arrest
- Operating room: 81.6%
- Labor ward: 10.3%
- Post-anesthesia care unit: 4.6%
Major causes of maternal cardiac arrest
-
Obstetric hemorrhage
The leading cause of MCA:
- Accounts for 40.2% of cases
- Often associated with:
- Placenta accreta spectrum (PAS)
- Placental abruption
- Surgical complications
Clinical significance:
Despite lower ROSC rates compared to AFE, patients who achieved ROSC after hemorrhagic arrest had excellent survival outcomes.
-
Amniotic fluid embolism (AFE)
Second most common cause:
- Represents 31% of cases
- Rapid onset, often within minutes of delivery
- Characterized by:
- Cardiovascular collapse
- Coagulopathy
- Hypoxemia
-
Anesthesia-related complications
Account for 11.5% of cardiac arrests
Most common mechanisms:
- High neuraxial block (6 cases)
- Bezold–Jarisch reflex
- Difficult airway and failed intubation
- Epidural dosing complications
-
Other causes
- Acute cardiac events (e.g., myocardial infarction)
- Respiratory failure
- Venous thromboembolism
- Trauma
- Air embolism
Anesthesia-related cardiac arrest: clinical insights
The study highlights critical anesthetic risks:
High neuraxial block
- Excessive spread of spinal/epidural anesthesia
- Leads to:
- Hypotension
- Respiratory paralysis
- Cardiac arrest
Risk scenarios
- Conversion of labor epidural to cesarean anesthesia
- Combined spinal-epidural techniques
- Emergency cesarean delivery
Risk factors for maternal cardiac arrest
Demographic risk factors
- Age ≥ 40 years → 6.6× higher risk
- BMI ≥ 40 kg/m² → ~3× higher risk
- Black and Asian/Pacific Islander race → increased risk
Clinical risk factors
The strongest associations included:
- Pulmonary hypertension (aOR 41.6)
- Placenta accreta spectrum (aOR 31.6)
- Ischemic heart disease (aOR 19.9)
- Stillbirth
- Hypertension and diabetes
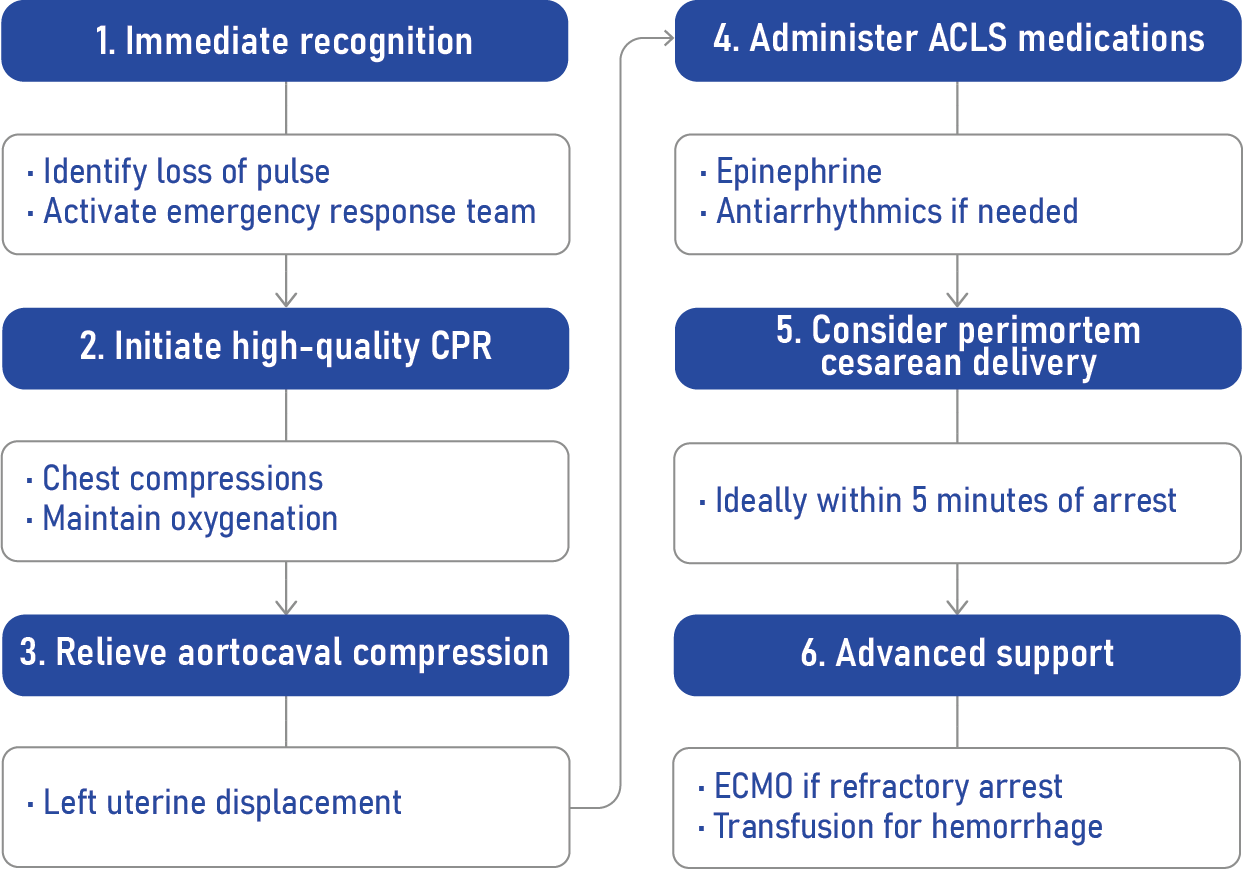
Management of maternal cardiac arrest
Core principles
Management follows modified ACLS protocols for pregnancy, with key adaptations:
- Left uterine displacement
- Early airway management
- Rapid identification of reversible causes
Interventions used in the study
- Epinephrine: 87.4%
- Sodium bicarbonate: 52.9%
- Blood transfusion: 50.6%
- Central venous access: 35.6%
- ECMO or cardiopulmonary bypass: 16.1%
Step-by-step emergency management
Deviations from guidelines
The study identified 18.4% of cases with deviations from recommended protocols:
Common issues
- Incorrect epinephrine dosing
- Delayed medication administration
- Delayed resuscitative cesarean delivery
Critical observation
- Only 5 out of 13 perimortem cesareans were performed within 5 minutes
Outcomes and prognosis
Survival statistics
- ROSC achieved: 77%
- 30-day survival: 67.8%
By etiology
- AFE: higher ROSC (85.2%)
- Hemorrhage: lower ROSC but strong survival after resuscitation
Long-term morbidity
- 5% required tracheostomy or gastrostomy
- Median hospital stay: 6 days
Why this study matters
This research provides granular, real-world data not available in administrative datasets.
Major contributions
- Detailed timing of cardiac arrest
- Specific anesthetic causes identified
- Real-world adherence to guidelines
- Identification of modifiable risk factors
Conclusion
Maternal cardiac arrest during anesthetic care remains rare but highly consequential. This landmark study reinforces that:
- Most cases are linked to hemorrhage and embolic events
- Anesthesia-related complications are significant but preventable
- Survival rates are encouraging when rapid, guideline-based care is delivered
Improving outcomes will depend on early recognition, strict adherence to ACLS protocols, and proactive management of obstetric risks.
Reference: Furdyna MJ et al. Frequency and Management of Maternal Peripartum Cardiac Arrest during Anesthetic Care: A Multicenter Retrospective Cohort Analysis. Anesthesiology. 2026;144:796-810.
Explore more about management of peripartum cardiac arrest in NYSORA’s Anesthesiology Manual. And for a digital learning experience, check out the Anesthesiology Module on NYSORA360!