
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Anesthetic management of medical problems in obstetric patients
- Safe obstetrical general anesthesia
- Methods of pain relief during labor
Definition and mechanisms
- Pregnant women may need anesthesia at any stage of gestation due to incidental surgery (e.g. appendicitis), trauma, delivery, or complications in the immediate postnatal period (e.g. bleeding, breast abscess)
- As pregnancy progresses, multisystemic physiological changes develop rapidly
- The obstetric anesthesiologist must understand these to provide optimum care to pregnant women
- Consider:
- Significant cardiovascular or cerebrovascular disease
- Significant respiratory disease, which may worsen throughout pregnancy
- Morbid obesity (BMI >40) or super morbid obesity (BMI >50)
- Significant hematological disease which may previously have resulted in failure to reach viable gestation
- Corrected or palliated congenital heart disease
- Be aware that pregnant patients are more sensitive to the effects of general anesthesia than non-pregnant patients
Anesthetic management of medical problems in obstetric patients
- Acquired cardiac disease
- Ischaemic heart disease (obesity and advanced age is increasingly seen in the obstetric population)
- Aortic dissection
- Cardiomyopathy
- Symptomatic valvular heart disease
- Sudden adult death syndrome (SADS)
- Antenatal management:
- Assess symptoms and functional status (NYHA class)
- Review recent ECG and echocardiography
- Multidisciplinary planning for labor and delivery
- Labor and delivery:
- Perform continuous maternal monitoring with ECG and invasive blood pressure monitoring for high-risk patients
- Provide epidural analgesia
- Be aware of the hypertensive response to laryngoscopy in case of general anesthesia
- Postnatal management:
- Be cautious with uterotonic agents due to side effects
- Perform hemodynamic monitoring during the first 24 hours because of the risk of decompensation with autotransfusion postpartum
- Congenital cardiac disease
- Maintain preload
- Avoid prolonged fasting
- Administer IV fluids
- Maintain afterload
- Avoid spinal anesthetic
- Administer phenylephrine for hypotension (or noradrenaline in on-responders)
- Administer oxytocin slowly (2 units/minute)
- Avoid tachycardia
- Administer effective analgesia
- Perform early cardioversion for any tachyarrhythmia
- Keep pulmonary vascular resistance low
- Administer oxygen
- Avoid hypercarbia by preventing sedation
- Maintain preload
- Neurological disease
- Stroke
- Subarachnoid hemorrhage
- Epilepsy
- Status epilepticus
- Multiple sclerosis
- Consider a theoretical risk of neurotoxicity to demyelinated nerves with regional anesthesia
- Myasthenia gravis
- Perform instrumental delivery as muscles fatigue quickly
- Regional anesthesia is preferred over general anesthesia
- Avoid magnesium as it can precipitate a myasthenic crisis
- Multiple sclerosis
- Respiratory disease
- Asthma
- Screen for pulmonary hypertension
- Asthma
- Hematological disease
- Increased risk of VTE, e.g. Factor V Leiden, antiphospholipid syndrome
- Increased risk of bleeding, e.g. von Willebrand’s disease, thrombocytopenias
- Reduced oxygen-carrying capacity, e.g. sickle cell disease, thalassemia, spherocytosis
- Regional anesthesia is safe to use but pay attention to the timing of anticoagulant if used
- Therefore, provide a recent assessment of platelet count in thrombocytopenia
- Back problems
- Spinal surgery
- Regional anesthesia is safe to use in most types
- Avoid scar sites
- Scoliosis surgery
- Avoid regional anesthesia in women with implanted rods
- Spina bifida
- Exclude tethered spinal cord
- Regional anesthesia can be applied at an unaffected level if tethered spinal cord is excluded
- Be cautious of accidental dural punctures
- Reduce the epidural volume as dural permeability is reduced
- Spinal surgery
Maternal-to-fetal transfer
| Medication class | Examples | Crossing of uteroplacental barrier? |
|---|---|---|
| Intravenous agents | Thiopental Propofol Ketamine | Yes |
| Inhalational agents | Isoflurane Sevoflurane Desflurane | Yes |
| Benzodiazepines | Midazolam Lorazepam | Yes |
| Opioids | Morphine Fentanyl Remifentanil | Yes |
| Neuromuscular blocking agents | Vecuronium Rocuronium Suxamethonium | No |
| Neuromuscular blocking reversal agents | Neostigmine Sugammadex | Yes Yes |
| Anticholinergic agents | Atropine Glycopyrrolate | Yes Yes |
Obstetric general anesthesia
- Pre-OR preparation
- Airway assessment
- Fasting status
- Antacid prophylaxis
- Intrauterine fetal resuscitation if appropriate
- Rapid sequence induction
- Check airway equipment and IV access
- Optimize position: head up + left uterine displacement
- Pre-oxygenate and consider nasal oxygenation
- Perform cricoid pressure
- Deliver appropriate induction and neuromuscular blocker doses
- Consider facemask ventilation
- 1st intubation attempt:
- If poor view of the larynx, optimize the attempt by:
- Reducing/removing cricoid pressure
- External laryngeal manipulation
- Repositioning head/neck
- Using bougie/stylet
- Verify successful tracheal intubation or if the intubation attempt fails, ventilate with a facemask
- If poor view of the larynx, optimize the attempt by:
- 2nd intubation attempt:
- Consider:
- Alternative laryngoscope
- Remove cricoid pressure
- Verify successful tracheal intubation or if the intubation attempt fails, ventilate with a facemask
- Consider:
- Declare failed intubation:
- Priority is to maintain oxygenation
- Supraglottic airway device
- Facemask – oropharyngeal airway
- Priority is to maintain oxygenation
- Further management: see non-obstretic surgery
Pain relief during labor
- During the first and early second stages of labor, visceral pain (mediated by the T10 to L1 spinal segments) is experienced
- This is usually felt in the abdomen, sacrum, and back
- In the latter part of the first stage and into the second stage, somatic pain (mediated via T12-L1 and S2-4) is experienced
- This is located in the vagina, rectum, and perineum
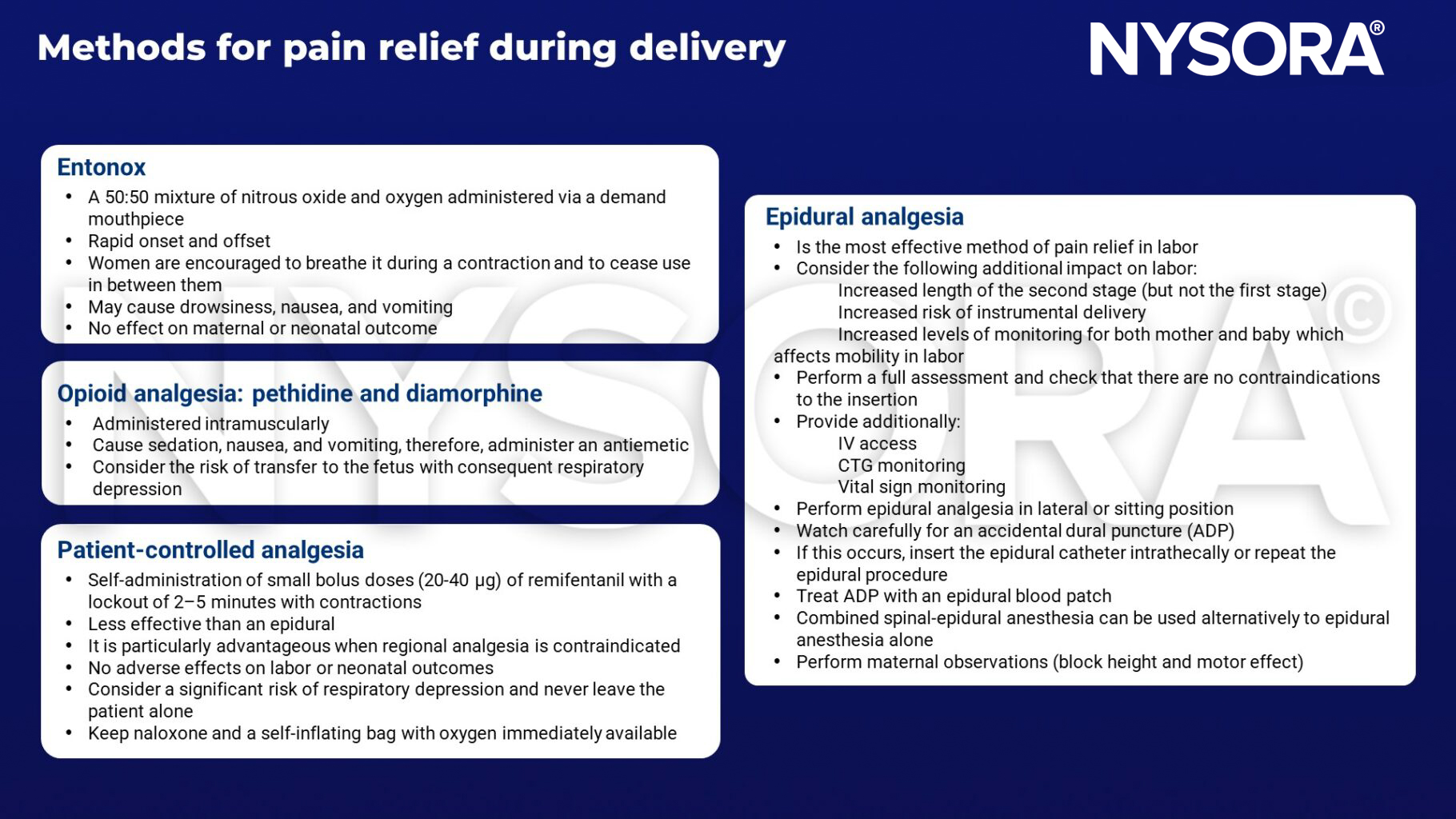
Methods for pain relief during labor
See caesarean delivery for anesthesia
Suggested reading
- Delgado, C., Ring, L., Mushambi, M.C., 2020. General anaesthesia in obstetrics. BJA Education 20, 201–207.
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.











