Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About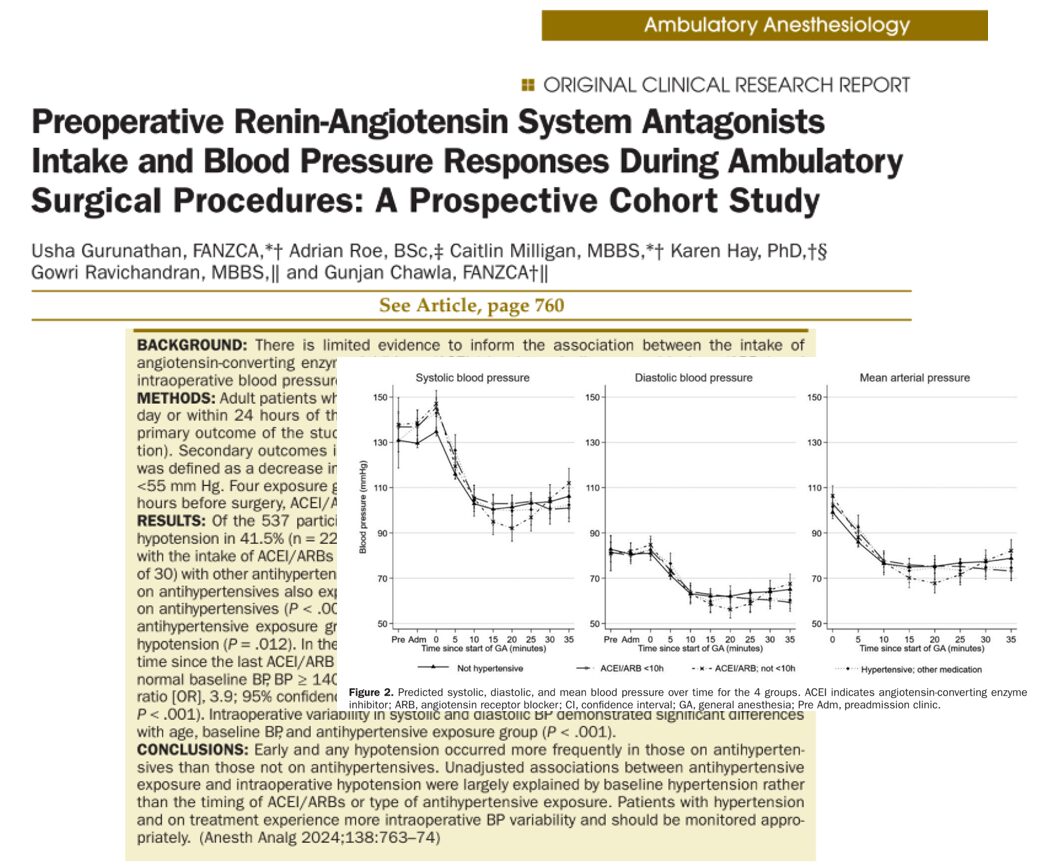





Ambulatory surgeries now constitute a significant and growing proportion of all surgical procedures, driven by advances in anesthesia, surgical technique, and perioperative care protocols. These procedures, often performed in otherwise healthy patients or those with stable chronic conditions, aim to maximize efficiency and minimize postoperative complications. However, the rising complexity of ambulatory patients, many of whom are elderly and hypertensive, necessitates a careful reevaluation of perioperative medication management, particularly antihypertensive therapies.
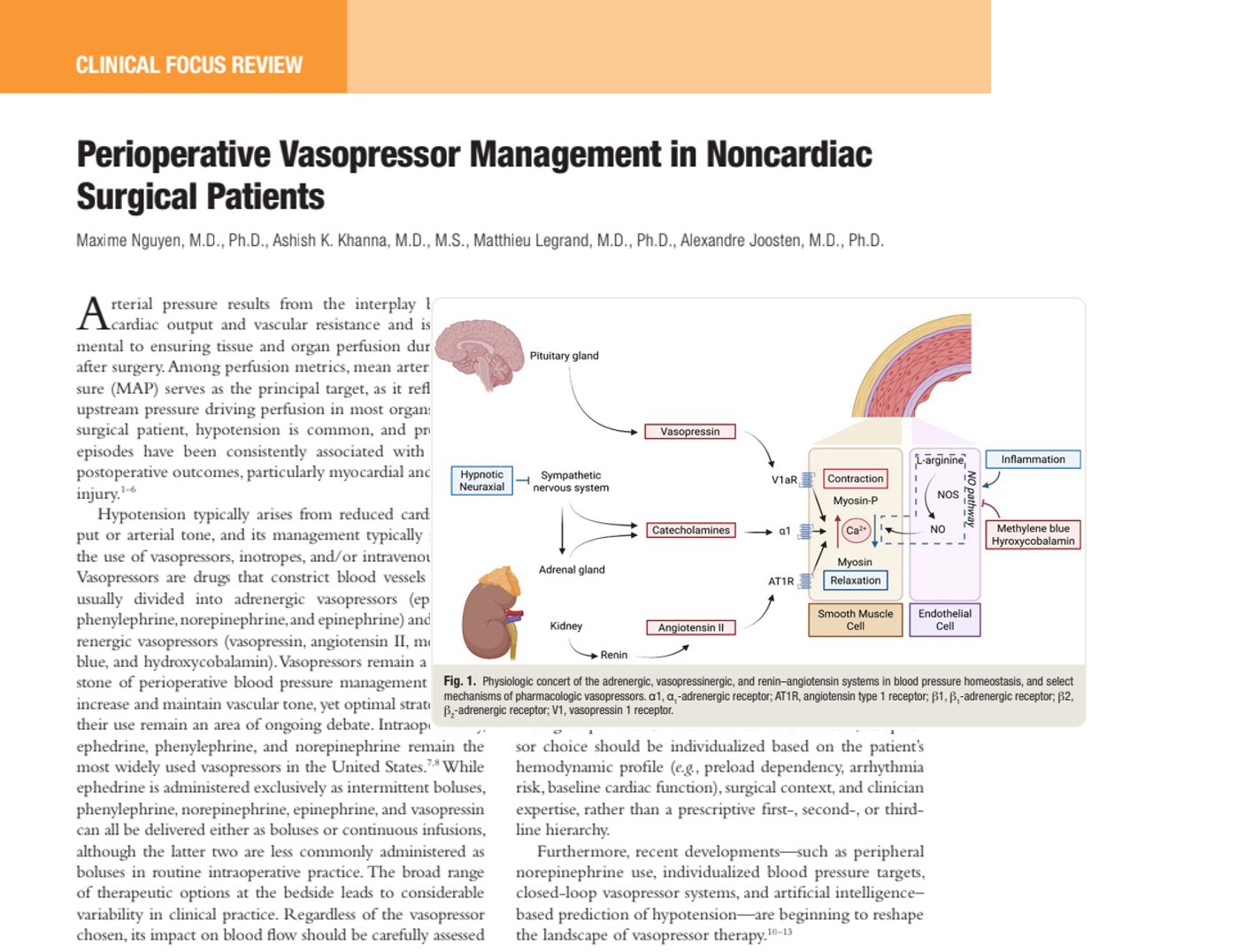
Among these, angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs) have been the subject of ongoing debate in perioperative medicine. These agents modulate the renin-angiotensin-aldosterone system (RAAS), playing a critical role in long-term blood pressure control. Yet, their vasodilatory effects and suppression of compensatory sympathetic activity can lead to intraoperative hypotension (IOH), especially during the induction phase of general anesthesia when sympathetic tone drops precipitously.
Recognizing this risk, major perioperative guidelines have issued varying recommendations:
- The American College of Cardiology/American Heart Association (ACC/AHA) 2014 guideline suggests withholding ACEIs/ARBs on the day of surgery due to the potential for refractory hypotension, especially in high-risk surgeries or those requiring significant fluid shifts.
- The European Society of Anaesthesiology (ESA) guidelines have taken a more nuanced approach, recommending individualized decisions based on procedure type, anesthesia modality, and patient comorbidities.
- Some institutional protocols routinely instruct patients to omit their ACEI/ARB dose on the morning of surgery, particularly in inpatient or major surgical settings, where the consequences of hypotension (e.g., renal injury, myocardial ischemia) may be more pronounced.
However, these recommendations are primarily based on data from major inpatient surgeries, such as cardiac, vascular, or large abdominal procedures. Ambulatory surgeries, characterized by lower hemodynamic stress and fluid shifts, have not been adequately represented in prior studies. This creates a critical knowledge gap: do the same concerns apply to low-risk, same-day procedures?
The prospective study by Gurunathan et al. (2024) seeks to fill this gap by examining the impact of ACEI/ARB continuation or cessation on intraoperative BP dynamics in ambulatory surgical patients. By focusing on the timing of antihypertensive intake, intraoperative BP variability, and short-term recovery outcomes, this research offers clinicians an evidence-based framework for medication management tailored to the ambulatory setting.
Study design overview
- Population: 537 adult patients undergoing ambulatory surgeries (609 procedures total).
- Setting: Two teaching hospitals in Queensland, Australia.
- Primary objective: To determine whether preoperative ACEI/ARB intake is associated with early intraoperative hypotension (IOH), particularly in the first 15 minutes of general anesthesia.
- Secondary outcomes: Any IOH throughout surgery, BP variability, length of PACU stay, and 24-hour postoperative recovery (QoR-15 score).
Key definitions
- Early hypotension: ≥ 30% systolic BP drop or MAP < 55 mmHg sustained for ≥ 5 minutes post-induction.
- Any hypotension: Meeting either threshold at any point during the surgical procedure.
- Exposure groups:
- Group A: Not on antihypertensives.
- Group B: On ACEI/ARB < 10 hours before surgery.
- Group C: On ACEI/ARB ≥ 10 hours before surgery.
- Group D: On non-ACEI/ARB antihypertensives.
Main findings
Hypotension prevalence
- Early IOH occurred in 25% of patients.
- Any IOH occurred in 41.5%.
- Among those not on antihypertensives (Group A), only 21% experienced early IOH, compared to:
- 30% (Group B),
- 41% (Group C),
- 30% (Group D).
Baseline hypertension: a stronger signal than timing
- Patients with baseline BP ≥ 140/90 mmHg had:
- 4x increased odds of early IOH.
- Nearly 8x increased odds of any IOH.
- This effect persisted even after adjusting for age and antihypertensive use.
The timing of ACEI/ARB intake showed no independent effect
- No statistically significant link between time since last ACEI/ARB dose and IOH incidence.
- Pharmacokinetic analysis using drug half-life units also found no association with MAP or SBP nadirs.
Blood pressure variability
- Greater systolic and diastolic BP variability was noted in patients:
- On antihypertensives, especially ACEI/ARBs.
- With higher baseline BP.
- Older in age.
Recovery metrics
- QoR-15 scores showed minimal decline postoperatively.
- PACU stay did not differ significantly across exposure groups or hypotension status.
- No readmissions or complications were recorded within 24 hours.
Clinical interpretation
This study challenges the prevailing notion that ACEI/ARB continuation is inherently risky in low-acuity surgery. While ACEI/ARB use correlated with higher BP variability and hypotension frequency, these effects were explained by underlying hypertension, not the medication timing itself.
This is a pivotal distinction. Past studies advocating for ACEI/ARB discontinuation often analyzed high-risk or inpatient surgical populations. In contrast, ambulatory procedures involve shorter anesthetic durations, less fluid shift, and typically healthier patients.
Practical recommendations

Conclusion
This large prospective study suggests that hypertension status, rather than ACEI/ARB timing, is the primary driver of intraoperative hypotension during ambulatory surgery. The findings reinforce the need to tailor perioperative plans to individual risk profiles rather than applying uniform medication hold policies.
Given the negligible impact on recovery and the practicality of managing BP variability intraoperatively, clinicians may now feel more confident in continuing ACEI/ARB therapy up to the day of surgery in select ambulatory cases.
Reference: Gurunathan U et al. Preoperative Renin-Angiotensin System Antagonists Intake and Blood Pressure Responses During Ambulatory Surgical Procedures: A Prospective Cohort Study. Anesth Analg. 2024;138:763-774.
Read more about this topic in NYSORA’s Anesthesia Updates.