
Explore NYSORA knowledge base for free:
Explore NYSORA knowledge base for free:


Master your emergency diagnostics skills on the go!

Convenience meets excellence with immersive walkthroughs to the most commonly used POCUS techniques, accompanied by proprietary NYSORA learning aids and clinical pearls.
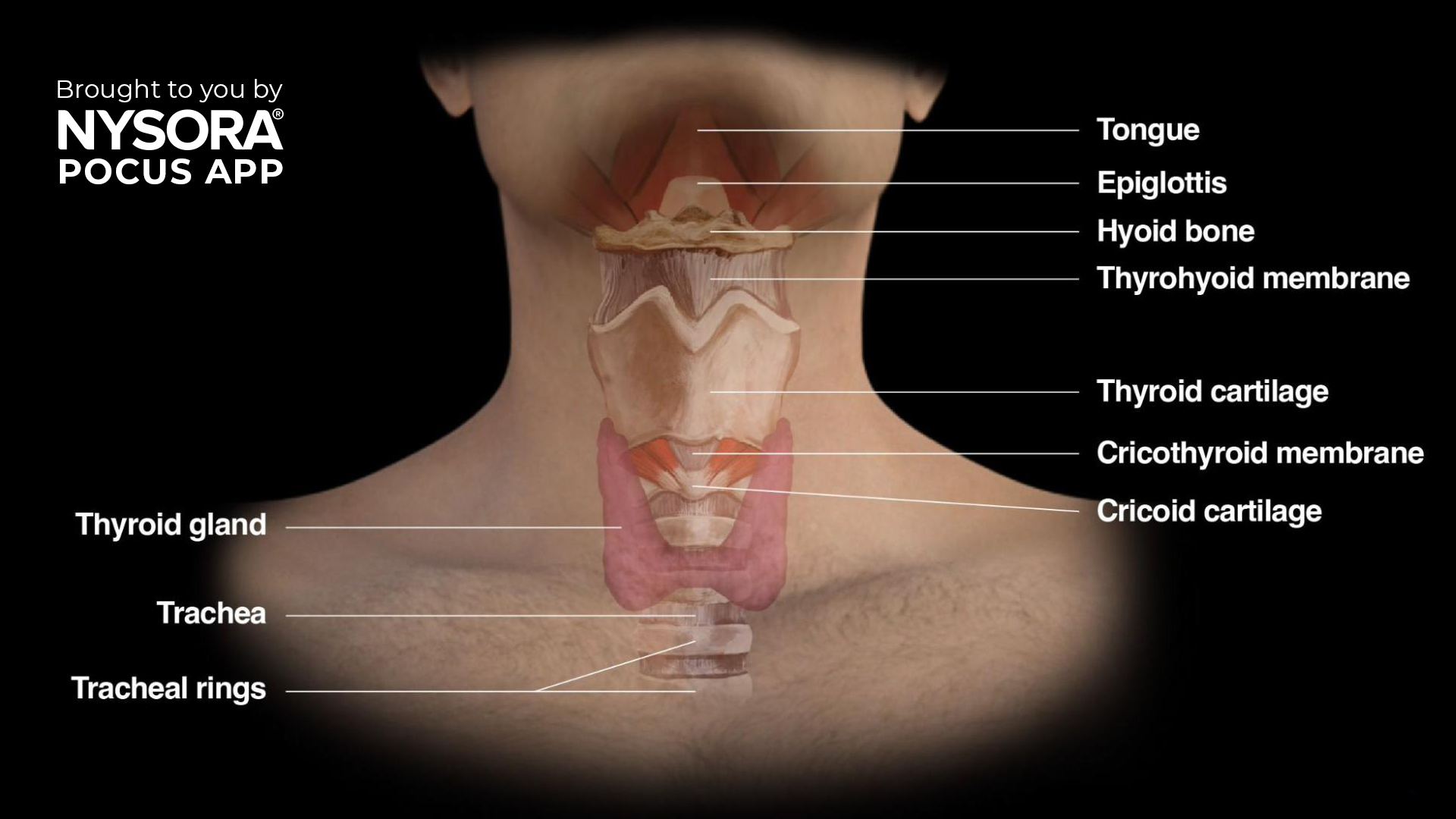
We are thrilled to announce the launch of our Airway Assessment course, now available in the POCUS App! This comprehensive course is designed to equip healthcare professionals with the knowledge and skills to perform advanced airway management using ultrasound techniques. Learning objectives You will gain expertise in: Understanding the anatomy and physiology of the upper airway. Identifying key upper airway structures. mastering the scanning techniques to assess the upper airway Why airway ultrasound? Safe and non-invasive: Quick and painless for patients. Highly accurate: Provides real-time assessment of airway structures and conditions. Improved outcomes: Reduces complications in difficult airway scenarios, a leading cause of anesthesia-related mortality. Evidence-based: Confirming ETT placement via ultrasound shows 98% sensitivity and specificity. What you’ll learn This course covers essential topics in airway ultrasound, including: Upper airway anatomy and physiology Gain a solid understanding of the functional anatomy. Identification of upper airway structures with ultrasound Detailed descriptions help you identify structures clearly, for instance: Hyoid bone – recognizable on ultrasound as a linear hyperechoic inverted U-shaped structure with two greater horns (cornua). Thyroid cartilage – ultrasound appearance as a hypoechoic inverted V-shaped or triangular structure. Cricothyroid membrane – appears as a hyperechoic horizontal line. Ultrasound imaging techniques Suprahyoid area Place the transducer longitudinally below the mandible and above the hyoid bone. Ultrasound image shows a fan-shaped tongue with a typical striated appearance. Underneath the mylohyoid and geniohyoid muscles, the tongue appears fan-shaped, with intrinsic muscles providing a striated appearance. Infrahyoid area: Sagittal ‘string of pearls’ technique Start from the trachea, sliding the probe cranially. The tracheal rings appear as dark hypoechoic structures, resembling a pearl necklace. Infrahyoid transverse approach Position the transducer transversely on the midline of the neck. Scan cranially to caudally, visualizing key landmarks: Hyoid bone Thyrohyoid membrane Thyroid cartilage Cricothyroid membrane Cricoid cartilage Trachea […]

The relationship between diabetes mellitus (DM) and delayed gastric emptying has long been a concern for anesthesiologists, especially due to the associated risks of pulmonary aspiration during surgery. A recent study by Sastre et al., published in the December 2024 issue of Anesthesia & Analgesia, provides new insights into this issue by investigating the prevalence of full stomach in diabetic patients with and without dysautonomia compared to healthy controls. This landmark research highlights the importance of preoperative gastric ultrasound in risk assessment and management. Key findings Background Delayed gastric emptying is a common concern in diabetic patients due to potential autonomic dysfunction. Traditional fasting guidelines do not always account for individual variations in gastric emptying, particularly in diabetics. Study overview Participants: 289 patients undergoing elective surgery: 83 diabetics with dysautonomia. 62 diabetics without dysautonomia. 144 healthy controls. Methodology: Preoperative gastric ultrasound was performed to assess gastric volume (GV) and content. The Perlas grading scale was used to classify gastric content. Results Prevalence of full stomach: Higher in diabetic patients with dysautonomia (22.9%) compared to diabetics without dysautonomia (16.1%) and controls (13.2%). Solid gastric residue: Observed in 12% of diabetics with dysautonomia, compared to 4.8% in those without and 3.5% in controls. Gastric volume: While antral cross-sectional area (CSA) was larger in dysautonomia-positive diabetics, residual GV was not significantly different among groups. Gastroparesis symptoms: Common in diabetics with dysautonomia but not a definitive predictor of full stomach. Implications for clinical practice Role of dysautonomia: The study underscores dysautonomia as a significant factor contributing to the presence of a full stomach, rather than diabetes alone. Utility of gastric ultrasound: Ultrasound is a reliable, non-invasive tool to assess gastric contents, enabling tailored perioperative management. Guideline reevaluation: Findings suggest that current fasting guidelines may not adequately address the unique risks in diabetics with dysautonomia. […]
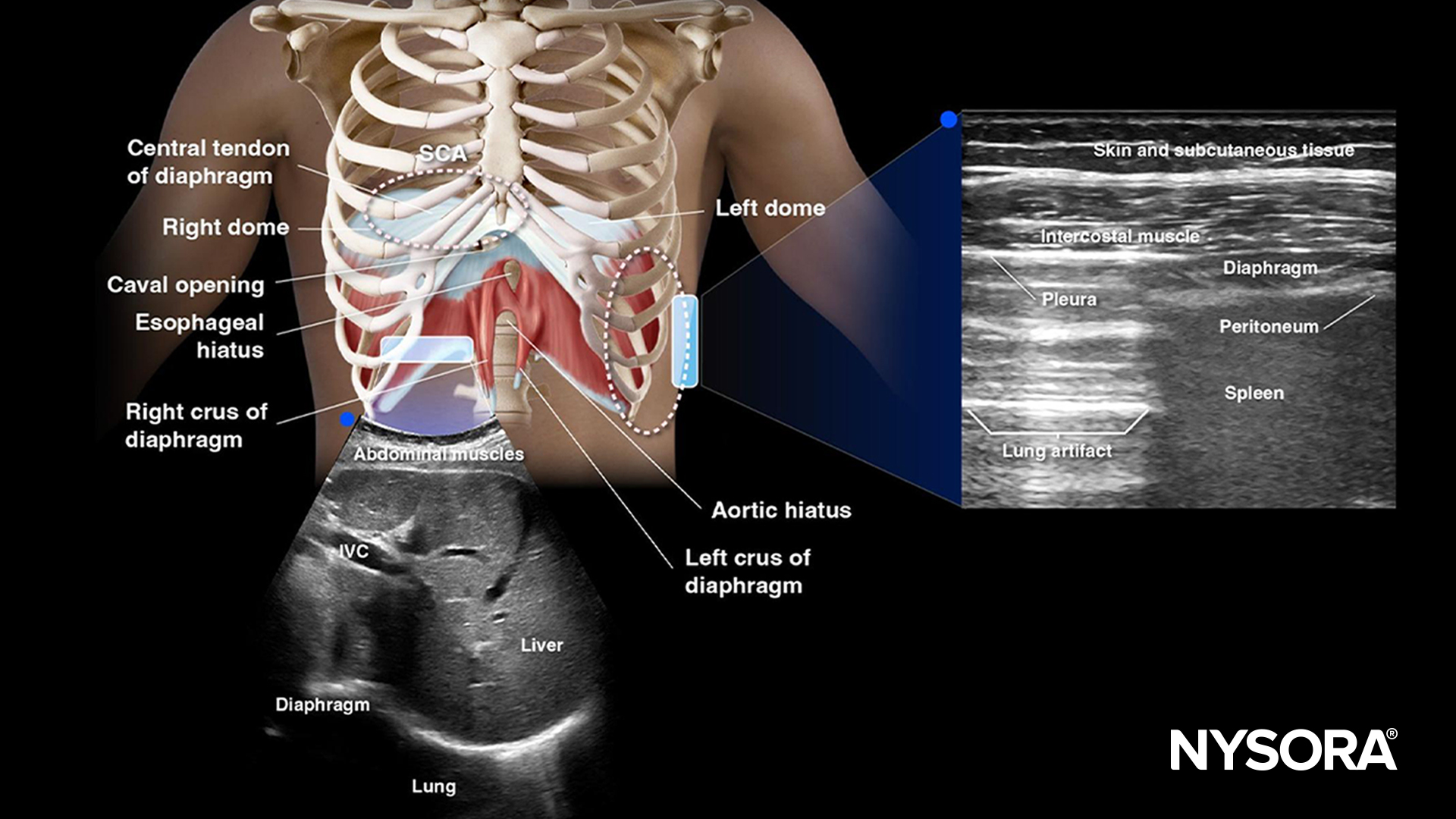
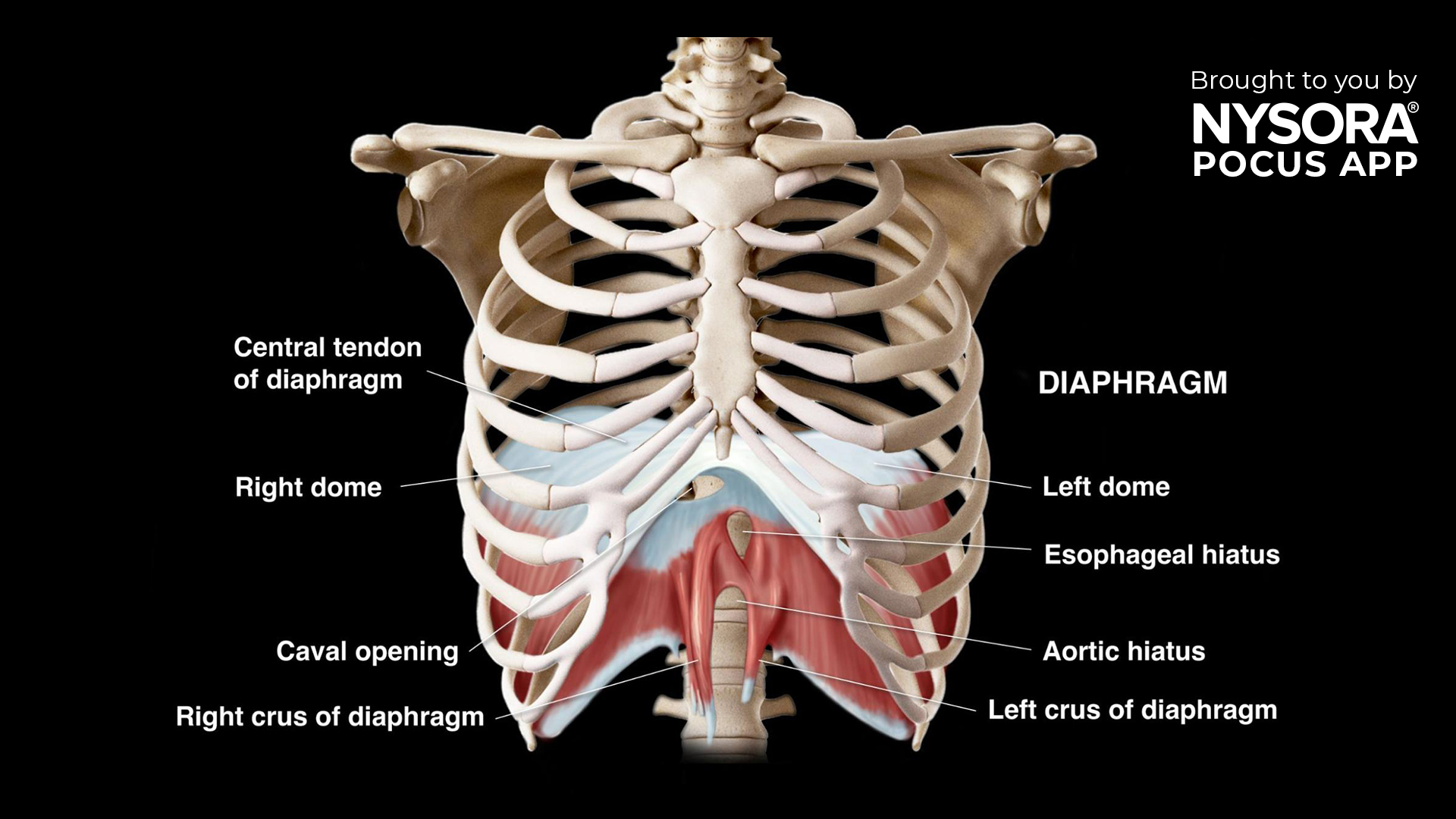
A recent study published in Regional Anesthesia and Pain Medicine (2024) introduces a novel approach to evaluating diaphragmatic function using point-of-care ultrasound (POCUS). Conducted by Dr. Diogo Da Conceicao and colleagues at Toronto Western Hospital, this research compares a novel method against two established techniques, highlighting its potential for enhanced diagnostic accuracy. Background The diaphragm, a crucial muscle for respiration, is often affected during certain medical procedures like brachial plexus blocks or surgeries involving the thoracic cavity. Traditional methods to evaluate diaphragmatic motion include: Excursion of the Dome of the Diaphragm (DOD): Uses a curvilinear transducer to measure motion through the abdomen by scanning the subcostal area. Thickening fraction of the Zone of Apposition (ZOA): Examines diaphragmatic thickening during inspiration with a linear probe. However, these methods face limitations: Left-side DOD measurements are challenging due to a narrow acoustic window. ZOA thickening measurements can be inconsistent due to variability in readings. To address these issues, the study explores measuring ZOA excursion via a high-frequency linear transducer placed at the mid-axillary line. Study design Participants: 75 elective surgical patients with normal diaphragmatic function. Exclusion criteria: abnormal pulmonary function, pre-existing diaphragm dysfunction, or BMI > 35 kg/m². Methods: Three ultrasound techniques were assessed: DOD excursion: Measured using a 2–5 MHz curved transducer. ZOA thickening fraction: Examined via a linear transducer in the lateral chest. ZOA excursion: Distance between end-inspiration and end-expiration of the ZOA’s uppermost point. Primary outcome: Success rate in capturing clear ultrasound views. Secondary outcomes: Procedure time and correlation among methods. Key findings High success rate for ZOA excursion: 100% success for both left and right sides compared to 98.7% (right) and 34.7% (left) for DOD excursion. ZOA excursion is unaffected by the narrow acoustic window that hampers DOD assessments. Procedure times: Median times for ZOA and DOD excursion measurements […]
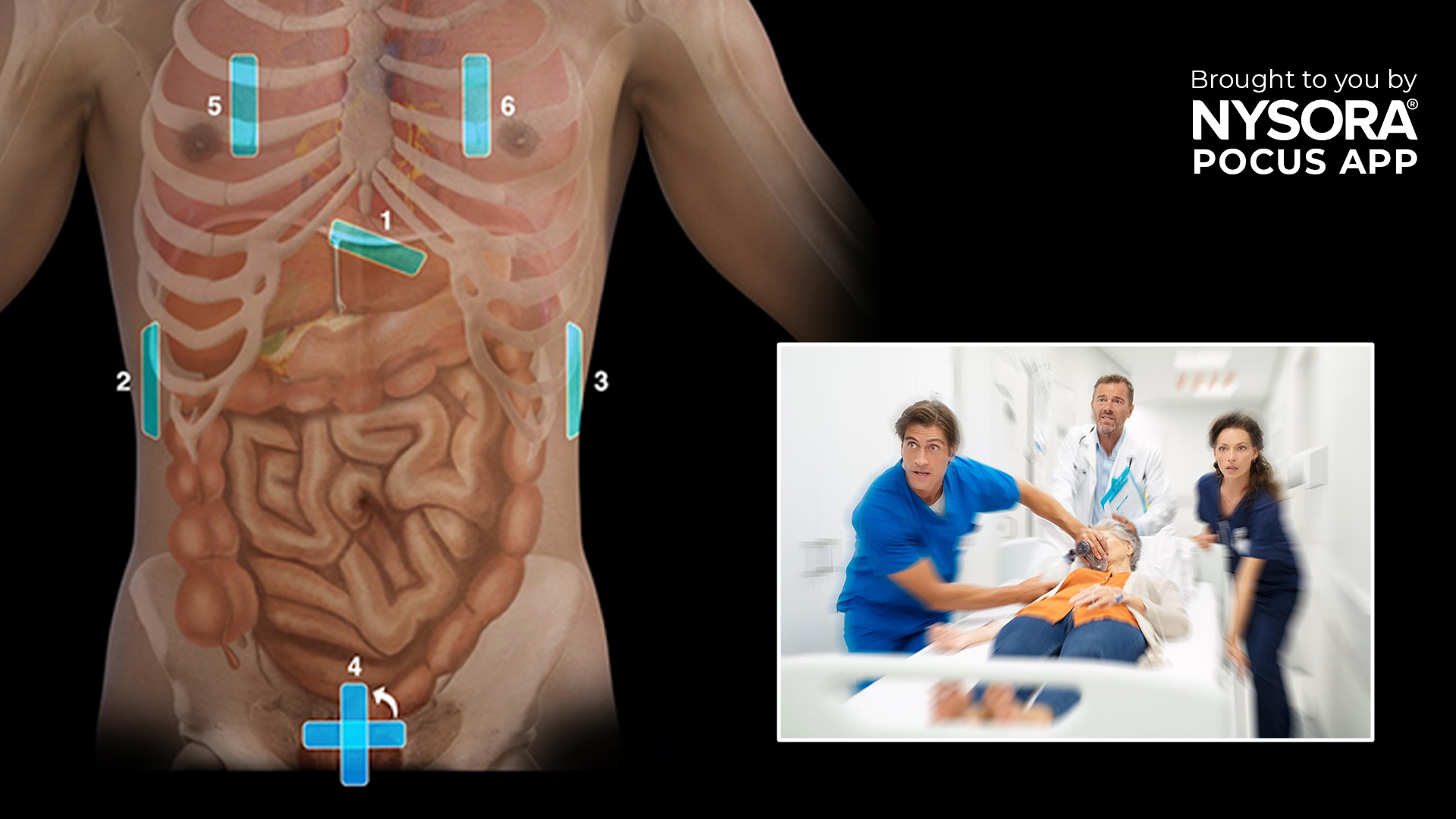
The extended Focused Assessment with Sonography in Trauma (eFAST) is a valuable diagnostic tool for quickly assessing trauma patients. It helps identify life-threatening conditions such as pneumothorax, cardiac tamponade, and intra-abdominal free fluid, which are common after blunt or penetrating trauma. Using point-of-care ultrasound (POCUS), eFAST allows healthcare providers to make rapid decisions about patient care, especially in the emergency department. What is eFAST? The FAST (Focused Assessment with Sonography in Trauma) exam was one of the earliest applications of POCUS and primarily focused on detecting free fluid in the abdomen. The eFAST exam expands on this by including an evaluation of the lungs to detect pneumothorax or intrathoracic fluid, making it an essential tool for trauma cases. A positive eFAST exam in an unstable patient can prompt immediate surgical intervention to prevent further deterioration. Key indications for eFAST: Pneumothorax: Collapsed lung that may cause breathing difficulties. Intrathoracic fluid: Accumulation of fluid in the chest cavity. Cardiac tamponade: Fluid accumulation around the heart leads to decreased cardiac output. Intra-abdominal free fluid: Blood or other fluid in the abdominal cavity, often indicating internal bleeding. Essential information about eFAST eFAST should be performed as part of the “C” (Circulation and Hemorrhage Control) in the ABC approach to trauma. eFAST can be used for both blunt and penetrating trauma, though the sensitivity in penetrating trauma improves with repeated scanning. A positive eFAST exam can indicate significant internal bleeding or trauma, which may require immediate surgery. Anatomy & fluid collection sites Intraperitoneal fluid tends to accumulate in specific anatomical locations due to gravity. These include: Morrison’s pouch: Between the liver and kidney. Perisplenic space: Around the spleen. Rectovesical pouch (in males) or rectouterine pouch (in females): Located in the pelvis, behind the bladder or uterus. eFAST examination technique Ultrasound machine setup: Transducer: Curvilinear or […]
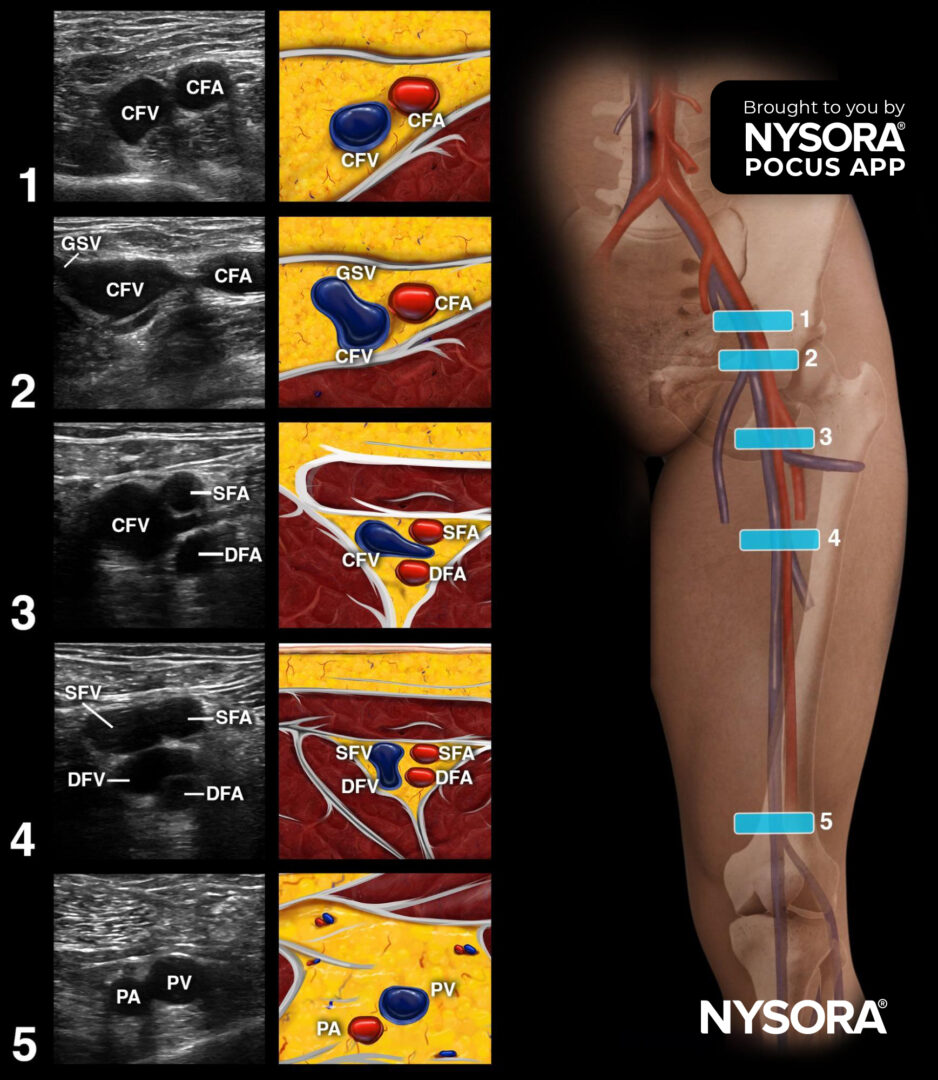
Deep venous thrombosis (DVT) is a serious medical condition in which a blood clot forms in the deep veins, typically in the legs. If left untreated, DVT can lead to life-threatening complications like pulmonary embolism (PE). This article presents a case study of a 52-year-old patient with DVT following recent orthopedic surgery. It outlines the steps for diagnosing and managing this condition using point-of-care ultrasound (POCUS) and clinical guidelines. A 52-year-old man presented to the emergency department with swelling and pain in his left leg, worsening over the last three days. Medical History: Recent knee replacement surgery (2 weeks ago) Obesity (BMI 33) Smoking habit (1 pack/day for 20 years) Clinical examination findings: Localized pain and asymmetric edema in the left leg. Reddish-blue skin discoloration over the calf. Mild dyspnea (shortness of breath) and discomfort in the chest, raising concerns about potential pulmonary embolism. Common risk factors for DVT: Recent surgery, especially orthopedic procedures Prolonged immobilization Cardiac conditions Hypercoagulable states (blood clotting disorders) Smoking, obesity, and use of contraceptive medications Diagnostic approach: Using POCUS to detect DVT Position the patient: Start with the patient supine with the leg extended and externally rotated. For popliteal (behind the knee) assessments, position the leg in flexion. 2. Scanning: Start at the inguinal crease with a linear transducer. Scan slowly and assess the compressibility of the vein every 1-2 cm along the femoral and popliteal areas. 3. Key locations for detecting thrombi: Common femoral vein (CFV) Bifurcation of the CFV and saphenous vein Popliteal vein Pay special attention to these regions as they are common sites for clot formation. 4. Confirm DVT: The vein’s non-compressibility is a definitive sign of DVT. In normal cases, applying pressure to the vein with the transducer should collapse it completely. If it remains open, a thrombus […]
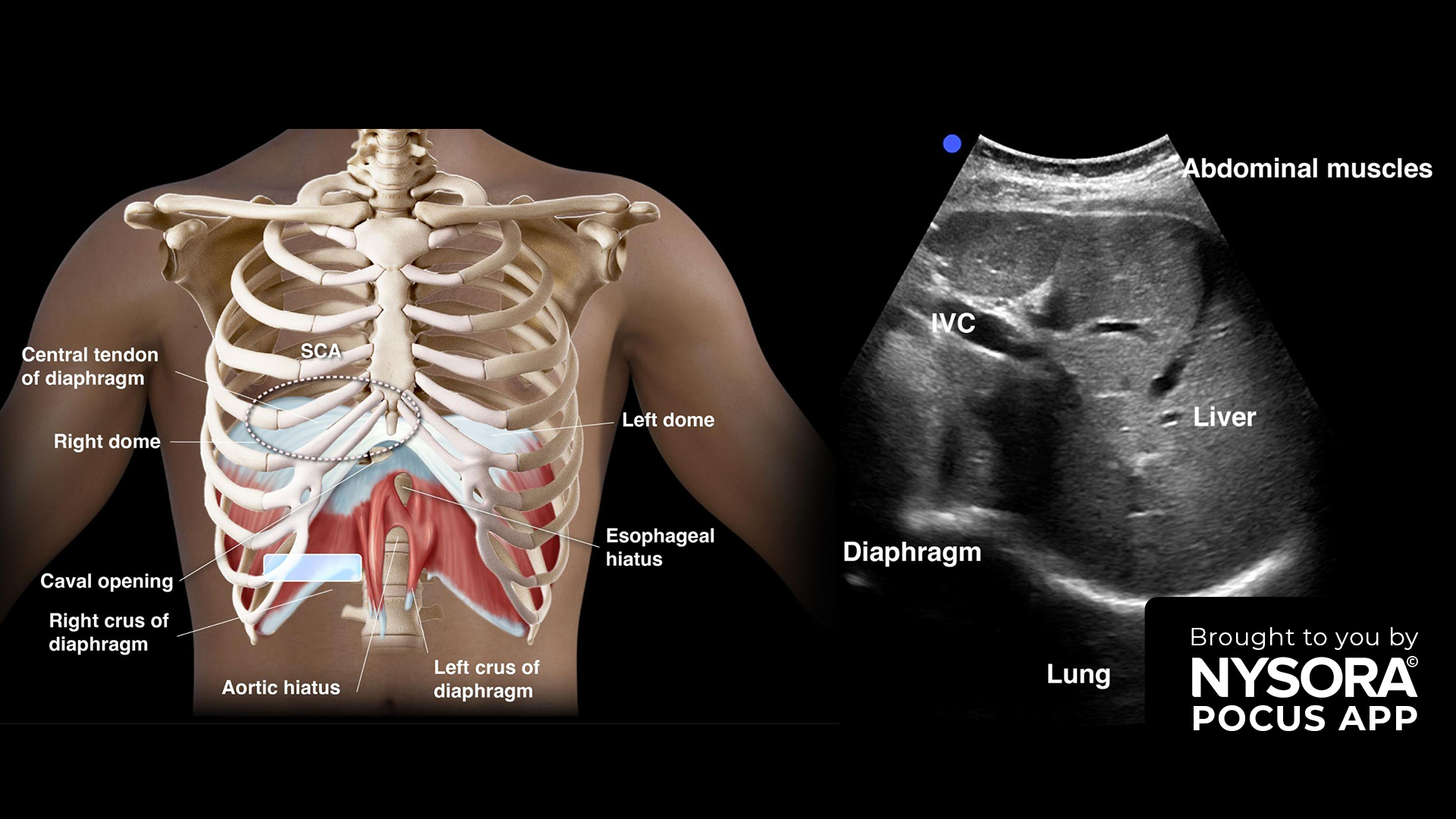
Diaphragm ultrasound is a non-invasive, point-of-care ultrasound (POCUS) technique used to assess diaphragmatic function. This case study explores its application in evaluating diaphragmatic dysfunction in a clinical setting. Case presentation A 60-year-old woman was transferred to the ICU following an elective cardiac surgery. Her medical history included chronic obstructive pulmonary disease (COPD) and hypertension. Postoperative complications included prolonged ventilator dependency and difficulty weaning from mechanical ventilation. Physical examination The patient was alert but exhibited signs of respiratory distress, including shallow breathing and accessory muscle use. Auscultation revealed reduced breath sounds at the lung bases. There was no evidence of overt neuromuscular weakness, but diaphragmatic dysfunction was suspected. Clinical decision Given the suspicion of diaphragmatic dysfunction contributing to the patient’s difficulty in weaning from mechanical ventilation, a diaphragm ultrasound was performed at the bedside to assess the diaphragm’s structure and function. Indications for diaphragm ultrasound Difficulty in weaning from mechanical ventilation Suspected diaphragmatic paralysis or dysfunction Postoperative assessment following high-risk surgeries Evaluation of neuromuscular disorders affecting respiratory function Essential information on diaphragm ultrasound Diaphragm ultrasound provides real-time, dynamic assessment of diaphragm movement and thickness. It is a bedside, non-invasive technique that offers immediate insights into diaphragmatic function. While it complements other imaging modalities, diaphragm ultrasound is particularly useful for trending diaphragm function over time. Ultrasound machine setup Transducer: Curvilinear or phased array SCA; linear for ZOA. Preset: Abdominal Orientation: Transverse for SCA and toward the head for ZOA. Depth: 12-18 cm for SCA; 1.5-3 cm for ZOA Patient Positioning Position the patient supine with both arms at their sides. For better access to the diaphragm, slight lateral decubitus or slight upright positioning may be utilized, though reproducibility may be lower. Landmarks Clavicle: Midclavicular line Axilla: Anterior axillary line Costal Margin: Identify for transducer placement Xiphoid Process: As a reference point for […]
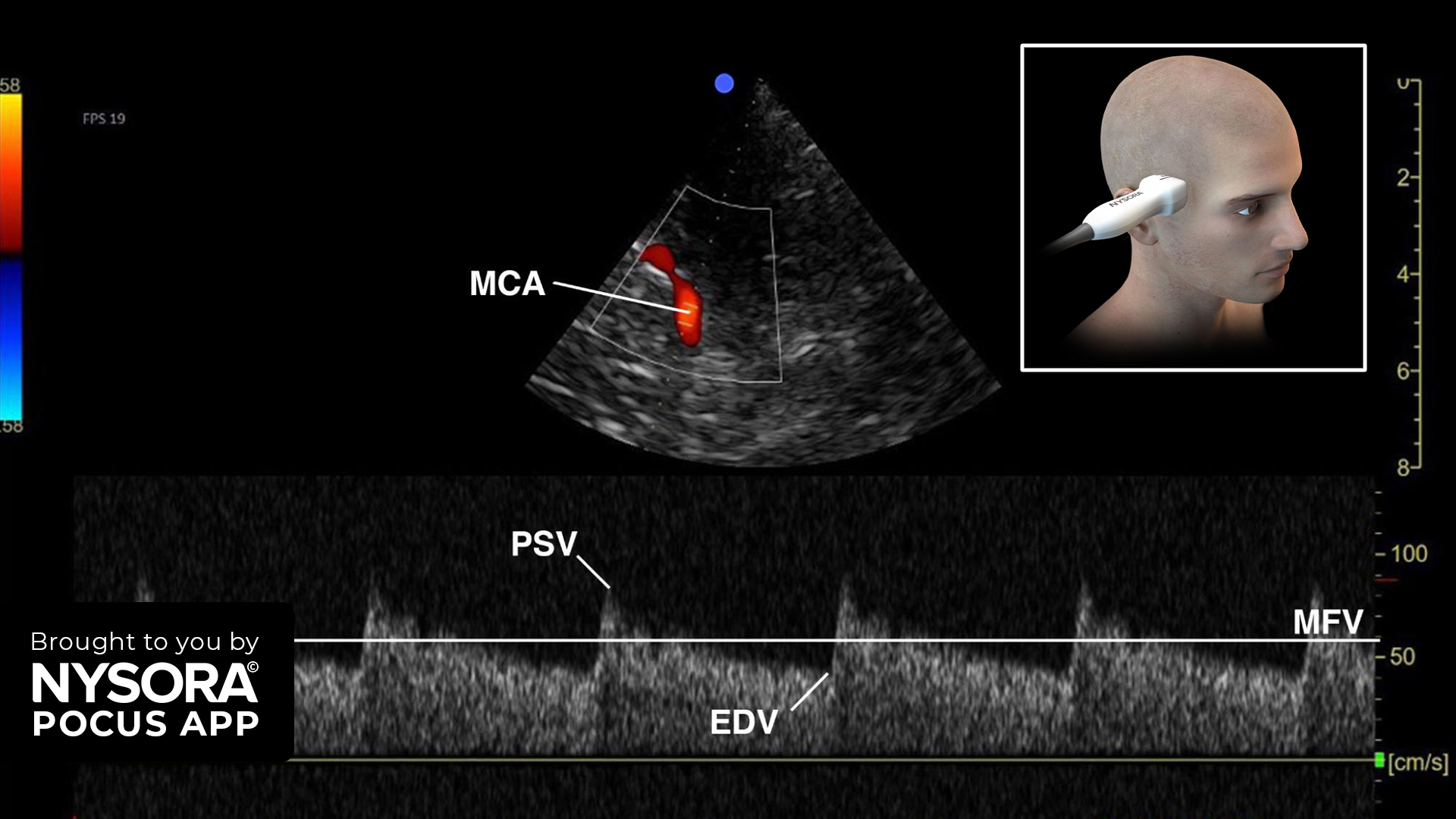
Transcranial Doppler (TCD) ultrasound is a non-invasive tool utilized in point-of-care ultrasound (POCUS) for assessing cerebral blood flow dynamics. This case study explores the application of TCD in detecting intracranial hypertension in a clinical setting. Case presentation: A 45-year-old male presented to the emergency department with severe headache, nausea, and blurred vision. Medical history included hypertension and a recent head trauma from a minor car accident. Physical Examination: The patient was conscious but exhibited signs of increased intracranial pressure (ICP), such as papilledema and bradycardia. Initial neurological assessment showed no focal deficits. Clinical Decision: Given the suspicion of intracranial hypertension, a TCD ultrasound was performed at the bedside to quickly assess cerebral blood flow dynamics and evaluate for raised ICP. Indications for TCD Intracranial hypertension Suspected diagnosis of cerebral circulatory arrest Vasospasm detection Identification of midline shift Essential Information on TCD TCD offers real-time information and can be performed at the bedside. It is not a replacement for CT scans but provides trending capabilities and immediate data. Functional Anatomy and Machine Setup Anatomy: Key structures include the circle of Willis and intracranial arteries. The mesencephalic plane is critical for vascular assessment. Machine Setup: Transducer: Phased array Preset: Transcranial (or cardiac) Orientation: Index marker toward the frontal bone/orbital Depth: 15 cm Patient Positioning: Patient positioned supine with the head of the bed elevated to 30 degrees. Landmarks include the ear and temporomandibular joint. Transducer placed 2-3 cm above the temporomandibular joint at the level of the temporal bone. Scanning Plane: Mesencephalic plane: Visualizes the middle cerebral artery (MCA) with red flow toward the transducer. Use pulsed wave Doppler to measure cerebral blood flow velocities. Assessment Using TCD Pulsatility Index (PI): Calculated using the formula: PI = (PSV – EDV)/ MFV Where PSV is peak systolic velocity, EDV is end diastolic velocity, and MFV […]
Accurate evaluation of fluid status in intubated, critically ill patients is crucial for effective patient management. Both hypovolemia and fluid overload can lead to adverse outcomes. Assessing fluid responsiveness—identifying patients who will benefit from volume administration—is essential in these settings. Carotid ultrasound has emerged as a novel, noninvasive method for predicting fluid responsiveness. This systematic review aims to update the literature on carotid ultrasound’s accuracy in predicting fluid responsiveness in mechanically ventilated patients. Carotid ultrasound, also known as carotid duplex ultrasound, is a noninvasive imaging technique used primarily to evaluate the structure and function of the carotid arteries. These arteries, located on either side of the neck, are vital as they supply blood to the brain,neck, and face. Carotid ultrasound combines traditional ultrasound with Doppler ultrasound to visualize the carotid arteries and assess blood flow. In recent years, carotid ultrasound has emerged as a novel tool for assessing fluid responsiveness in critically ill patients. Fluid responsiveness refers to the ability of a patient’s cardiovascular system to respond to fluid administration with a significant increase in stroke volume. This is particularly important in the management of patients in intensive care units (ICUs) or undergoing major surgery. Mechanism Carotid Doppler Peak Velocity (CDPV): Measures the peak velocity of blood flow through the carotid artery. Changes in CDPV can indicate changes in cardiac output and stroke volume in response to fluid administration. Corrected Flow Time (FTc): Assesses the time taken for blood to flow through the carotid artery, corrected for heart rate. FTc can provide insights into the filling status of the heart and fluid responsiveness. META-ANALYSIS OF CURRENT LITERATURE Carotid Ultrasound Parameters and Outcomes Common Parameters: Corrected Flow Time (FTc) Change in Carotid Doppler Peak Velocity (∆CDPV) Change in Carotid Artery Velocity-Time Integral (∆CAVTI) Common Cardiac Output Measures: Transthoracic Echocardiography (TTE) PiCCO […]
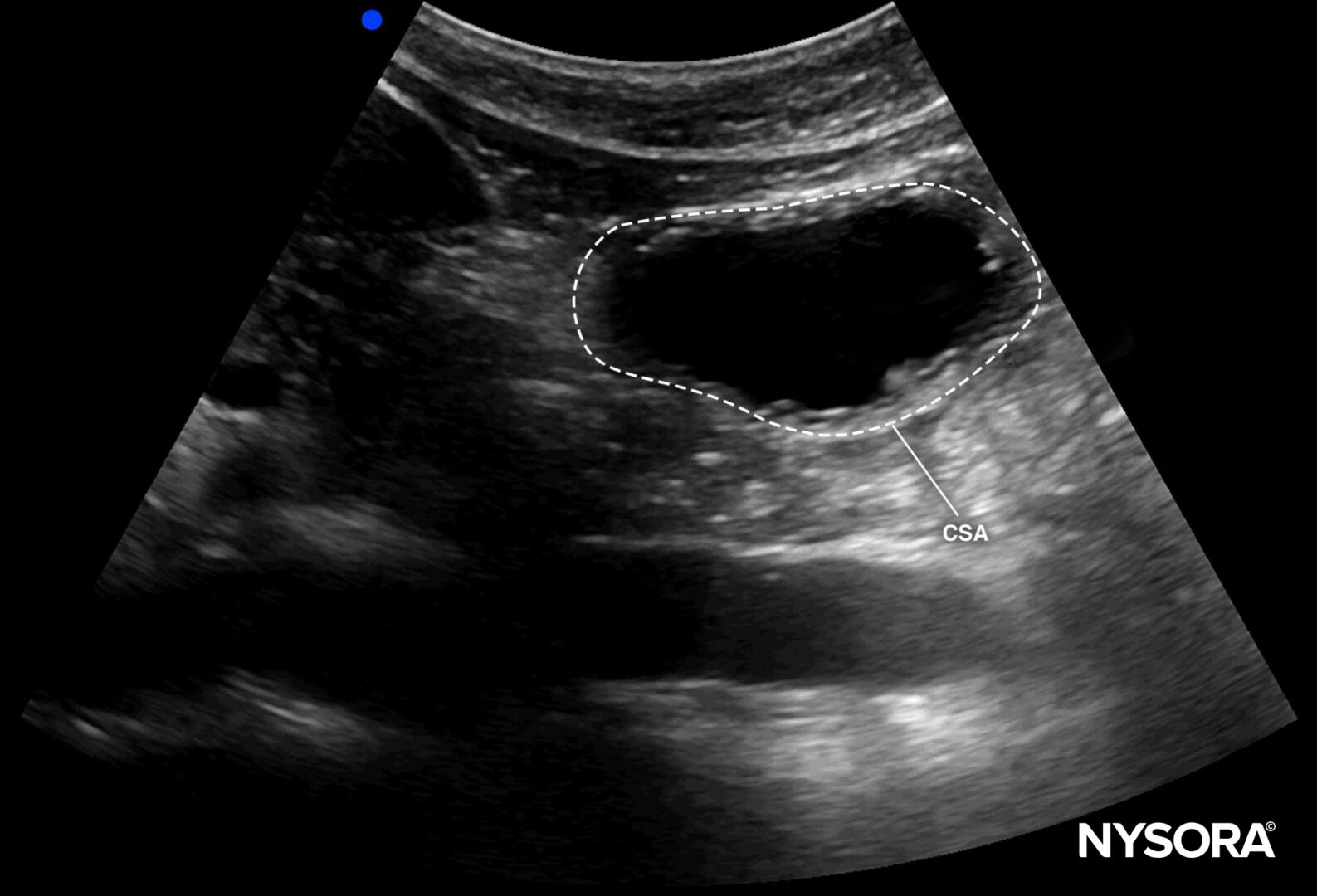
A recent meta-analysis underscores the importance of gastric ultrasound in anesthetic practice, particularly for assessing the risk of pulmonary aspiration due to gastric contents. This study aims to establish a reliable upper limit for normal gastric antral area and volume in fasting adults, providing crucial benchmarks for safer anesthesia management. The study analyzed data from 12 primary studies conducted between January 2009 and December 2020, encompassing 1,203 subjects. It determined that the 95th percentile for antral cross-sectional area (CSA) is 9.9 cm², and for gastric volume, it is 2.3 mL/kg. These values provide a critical benchmark for identifying patients at risk of aspiration. Distribution of values of the cross-sectional area measured in the right lateral decubitus position (left) and the gastric volume (right) for all patients. The blue line indicates the median and the red line indicates the 95th percentile value based on the Harrell-Davis method and bootstrap method, respectively. CSA, cross-sectional area. Historically, the threshold for high aspiration risk was set at a gastric volume of 0.8 mL/kg, based on animal studies. However, this meta-analysis reveals that this threshold is overly conservative. The findings suggest that the median gastric volume in fasting adults is approximately 0.6 mL/kg, with the 95th percentile reaching 2.3 mL/kg. The study’s results are significant for clinical practice. They suggest that a gastric antral area of 10 cm² in the right lateral decubitus position can serve as a practical upper limit for fasting patients. Furthermore, the data indicate that an antral grade of 0 or 1 (indicating an empty or nearly empty stomach) correlates with a 98% probability of having a gastric volume below the 95th percentile, thus significantly reducing aspiration risk. This research underscores the utility of gastric ultrasound as a non-invasive tool for evaluating gastric content at the bedside, especially when a patient’s […]

A 52-year-old male patient with a long-standing history of chronic shoulder dislocations presented for elective arthroscopic shoulder surgery. Given his history of recurrent shoulder instability, the surgical team anticipated significant postoperative pain, leading them to plan an interscalene brachial plexus block for postoperative analgesia. This type of block, frequently used for shoulder surgery, is known for its effective pain relief by anesthetizing the nerves that supply the shoulder. However, a common side effect of the interscalene block is phrenic nerve paresis, which can result in diaphragmatic dysfunction or paralysis. Understanding phrenic nerve paresis The phrenic nerve is responsible for innervating the diaphragm, the main muscle involved in breathing. Because of the close anatomical relationship between the phrenic nerve and the interscalene space, there is a significant risk that the nerve could be affected during the block, resulting in diaphragmatic paralysis. This complication, while typically temporary, can reduce the patient’s respiratory capacity and lead to discomfort, especially in patients with pre-existing lung conditions or obesity. In this case, to proactively manage the risk of respiratory complications, point-of-care ultrasound (POCUS) was used to monitor the patient’s diaphragm function before and after the block. Preoperative diaphragm assessment Before the block was administered, the anesthesia team used diaphragm ultrasound to assess the baseline function of the diaphragm. The subcostal view was selected as the primary scanning window, which allows for clear visualization of the diaphragmatic excursion (the movement of the diaphragm during the respiratory cycle). Baseline observation: Pre-block, excursions of 1 cm were measured during shallow breathing, indicating that the patient’s diaphragm was functioning properly. This baseline measurement is crucial for comparison with postoperative function to identify any potential changes. Postoperative diaphragm monitoring Following the administration of the interscalene block and the successful completion of surgery, POCUS was again utilized to assess any changes in diaphragmatic […]
Diaphragm dysfunction can arise from several causes, but for regional anesthesia practitioners, one of the most well-known is the interscalene block. This block, commonly used for shoulder surgeries, may inadvertently affect the diaphragm, leading to dysfunction on the blocked side. Immediate, non-invasive assessment of diaphragm function is vital for ensuring optimal patient care in these cases. We are excited to announce the launch of our newest course in the Point-of-Care Ultrasound (POCUS) app: Diaphragm Ultrasound. This course is designed to empower healthcare providers with the skills to evaluate diaphragm function at the bedside quickly and accurately. Course highlights: 30+ Original illustrations and animations: Each lesson contains high-quality visuals, enhancing understanding of diaphragm ultrasound techniques. Practical learning approach: Step-by-step guides, from machine setup to interpretation, ensure a hands-on experience in diaphragm assessment. Non-invasive techniques: Learn non-invasive approaches immediately applicable in clinical settings for evaluating diaphragm function. This course delivers essential background information alongside practical skills to fully grasp diaphragm anatomy, functionality, and its importance in medical practice. Whether you’re preparing for surgery, monitoring postoperative patients, or managing ventilator weaning in the ICU, this course covers it all. Why is diaphragm assessment important? Diaphragm ultrasound is becoming increasingly relevant in various clinical settings due to its non-invasive nature, ease of use, and accuracy. It plays a critical role in: Preoperative assessment of patients at risk for phrenic nerve damage. Postoperative monitoring after high-risk surgeries, such as cardiothoracic or upper abdominal procedures. Critical care, particularly in ventilatory weaning to evaluate diaphragm atrophy or predict difficult weaning. Assessing neuromuscular disorders or respiratory diseases that may impact diaphragm function. Learning objectives By the end of this course, learners will be able to: Understand the anatomy and physiology of the diaphragm. Identify key structures in the diaphragm via ultrasound. Perform dynamic assessments of diaphragmatic function. Recognize […]
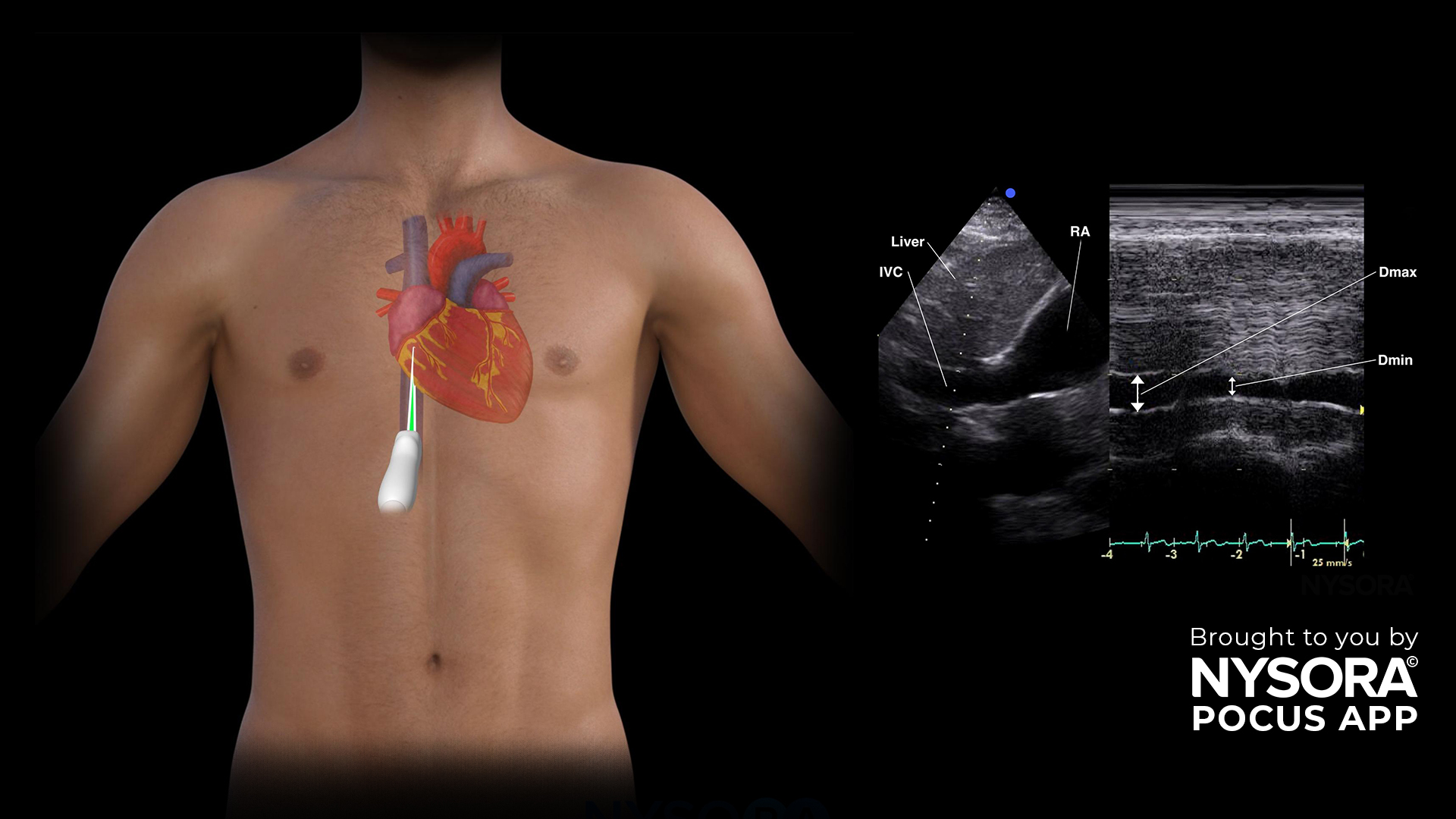
A 72-year-old patient was admitted to the Intensive Care Unit (ICU) for monitoring after traumatic brain injury. The patient is fully sedated, ventilated and requires norepinephrine for maintaining adequate cerebral perfusion pressures. He has no severe comorbidities and focused cardiac ultrasound showed normal biventricular function and valves. The patient is rather hypotensive and you are in doubt whether you should administer IV fluids. Here’s how POCUS can be used to assess the fluid status: Obtain a clear view of the inferior vena cava (IVC) using the IVC view. Use the M-mode 2 cm distal to its junction with the right atrium or 1 cm distal to the hepatic vein. First, assess the diameter of the IVC. The size is between 1.5 and 2.5 cm. Secondly, assess the minimal diameter and the maximum diameter with M-mode. Calculate the distensibility index: (max. diameter (Dmax) – min. diameter (Dmin))/min. diameter (Dmin) If it is >18%, this patient could benefit from fluid administration. Transform your practice with the power of POCUS using NYSORA’s POCUS App. Enhance your skills, broaden your diagnostic capabilities, and provide outstanding patient care. Experience the difference today – Download the app HERE.







POCUS is becoming the most reliable decision-making tool for diagnostics in emergency medicine and critical care. The POCUS app helps master it on your terms.



We recently partnered with Dr. Ray on POCUS. He is an anesthesiologist and critical care physician and he explains that the transition from regional anesthesia into POCUS is a natural step that considerably changes your practice. Therefore, we designed an app together to empower healthcare professionals with advanced guidance on POCUS wherever they go. We sat down with him to discuss POCUS, its history, and NYSORA’s role in the app publication.


The NYSORA POCUS (Point-of-Care Ultrasound) App is a mobile-friendly, expert-designed resource for healthcare professionals performing bedside ultrasound. It offers step-by-step protocols, high-quality ultrasound images, instructional animations, and clinical tips to optimize diagnostic accuracy and procedural confidence in emergency, critical care, and perioperative settings.
The app is ideal for anesthesiologists, emergency physicians, intensivists, internists, medical residents, and any healthcare professional utilizing POCUS for diagnosis and procedural guidance.
The objective of point-of-care ultrasound (POCUS) is to facilitate rapid clinical decision-making by providing real-time diagnostic information directly at the patient’s bedside. It allows healthcare providers to quickly assess patients, guide interventions, monitor treatment responses, and expedite patient care, particularly in critical or emergency situations.
The app includes:
The NYSORA POCUS App provides quick access to expertly-curated content, helping you:
Absolutely. The app is designed as a real-time reference tool, offering concise and structured guidance that can be used directly at the bedside.
NYSORA regularly updates the app to reflect the latest research, best practices, and clinical guidelines. Subscribed users receive these updates automatically, ensuring access to the latest updates and techniques.
Download the NYSORA POCUS App from your preferred app store, create an account, and explore the free content. For extended features, subscribe to unlock the full library and advanced tools.
Yes. The app includes high-quality instructional videos and animations demonstrating scanning techniques.
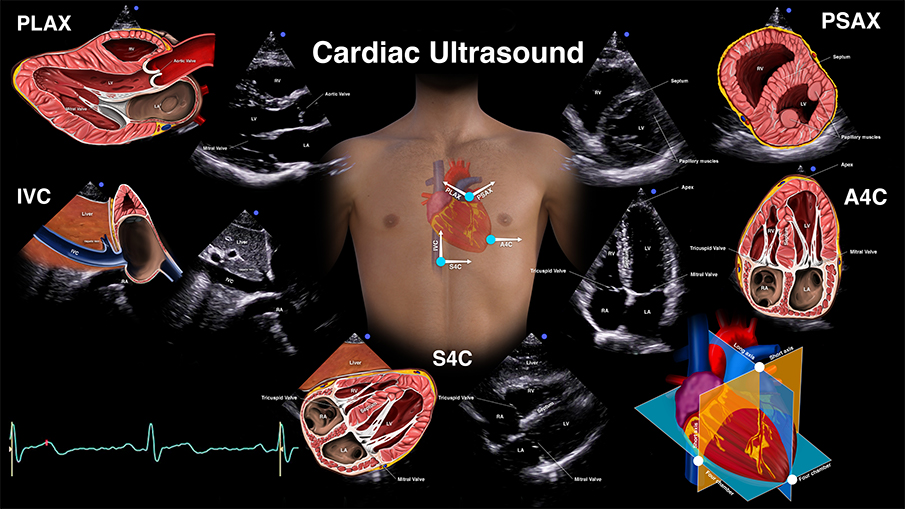
Yes. The app features detailed anatomical illustrations and NYSORA’s unique “reverse ultrasound anatomy” illustrations, helping you quickly recall sonographic patterns.
These are proprietary, revolutionary NYSORA educational tools. They take you from the ultrasound image to an illustrated anatomy view—and back again. This approach reinforces crucial anatomical knowledge and helps you recognize sonoanatomy patterns.
The app is designed to be highly practical, offering direct clinical applications and hands-on guidance for bedside ultrasound assessment and interventions.
Yes. The app includes interactive tools such as animations, videos, and self-assessment quizzes, making it easier to gain a thorough understanding and retain knowledge.
The app covers:
The app can be used in multiple ways:
1.Pre-scan review – Quickly review scanning protocols before performing an exam.
2.Live guidance – Follow step-by-step instructions while scanning.
3.Skill development – Improve diagnostic accuracy with expert insights and pathology recognition tools.
It’s a mobile-friendly reference tool offering:
The NYSORA POCUS App is developed by NYSORA’s team of experts. The content is rigorously reviewed and updated to provide evidence-based, clinically relevant information trusted by healthcare professionals worldwide.