Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the risk factors and symptoms of peripartum cardiomyopathy
- Diagnose peripartum cardiomyopathy
- Manage patients with peripartum cardiomyopathy
Background
- Peripartum cardiomyopathy (PPCM) is a rare cause of cardiomyopathy occurring during late pregnancy or in the early postpartum period
- Characterized by significant left ventricular dysfunction and heart failure in the peripartum period in the absence of other identifiable causes of heart failure
- Potentially life-threatening condition
- Left ventricle ejection fraction is nearly always less than 45%
- Etiology is unclear but likely multifactorial (hormonal, inflammatory, genetic,…)
Risk factors
- African descent
- Increasing age
- Pregnancy-related hypertension
- Multiparity
- Multiple gestations
- Obesity
- Chronic hypertension
- Chronic tocolytics use
- Cocaine use
Signs & Symptoms
- Paroxysmal nocturnal dyspnea
- Pedal edema
- Orthopnea
- Dyspnea on exertion
- Dry cough
- Palpitations
- Increase in abdominal girth
- Lightheadedness
- Chest pain
- Jugular venous distentions
- Displaced apical impulse
- Third heart sound
- Mitral regurgitation murmurs
Diagnosis
- Diagnosis is based on exclusion
- Differential diagnoses:
- Pulmonary embolism
- Severe sepsis
- Amniotic fluid embolism
- Preeclampsia/pregnancy-induced hypertensive disease
- Arrhythmias
- Severe anemia
- Myocardial infarction
- Dilated cardiomyopathy of other etiologies
- Diagnostic tests:
- Routine blood tests
- Evaluate for anemia, electrolyte abnormalities, endocrine conditions, renal or liver dysfunction
- Brain natriuretic peptide (BNP) is commonly elevated in patients with heart failure and PPCM
- Chest radiography
- Cardiomegaly and/or pulmonary edema are suggestive of heart failure but nonspecific to PPCM
- ECG
- Sinus tachycardia, supraventricular tachycardia, ventricular tachycardia, ST segment and T wave abnormalities, dilation of chambers, and QRS prolongation may be observed but are nonspecific
- Echocardiography
- Left ventricular ejection fraction <45%: Requirement for PPCM diagnosis
- Evaluation of other etiologies such as valvular diseases or structural abnormalities
- Ventricle/atrium dilation and left ventricular thrombus or atrial thrombosis may be present
- Cardiac MRI
- Evaluation of other causes of heart failure
- Cardiac catheterization
- Only for selected patients
- Left heart catheterization is indicated in patients with suspected ischemic cardiomyopathy
- Routine blood tests
Management
Management is similar to that of other causes of heart failure
- Pharmacological
- Angiotensin-converting enzyme (ACE) inhibitors: First-line treatment postpartum, contraindicated during pregnancy
- Hydrazaline and nitrate therapy can be used safely during pregnancy
- Beta-blockers
- Digoxin (carefully monitor plasma levels)
- Loop diuretics (e.g., furosemide)
- Avoid calcium channel blockers and aldosterone antagonists
- Thromboprophylactic low molecular weight heparin
- Non-pharmacological:
- Non-invasive ventilation or intubation
- Inotropic support
- Intra-aortic balloon pump, left ventricular assist device or extracorporeal membrane oxygenation may be required in severe cases
- Heart transplantation in severe cases who do not respond to therapy
- Implantable defibrillator or cardiac resynchronization in patients with chronic functional impairment
Prognosis
| Good prosnosis | Small left ventricular diastolic dimension (less than 5.5cm) |
| Left ventricular ejection fraction greater than 30% to 35% and fractioning of shortening greater than 20% at the time of diagnosis | |
| Absence of troponin elevation | |
| Absence of left ventricular thrombus | |
| Non-African ethnicity | |
| Poor prognosis | QRS greater than 120 ms |
| Delayed diagnosis | |
| High New York Heart Association (NYHA) class | |
| Multiparity | |
| African descent |
Complications
- Thromboembolism
- Arrhythmias
- Progressive heart failure
- Misdiagnosis as preeclampsia
- Fetal distress from hypoxia
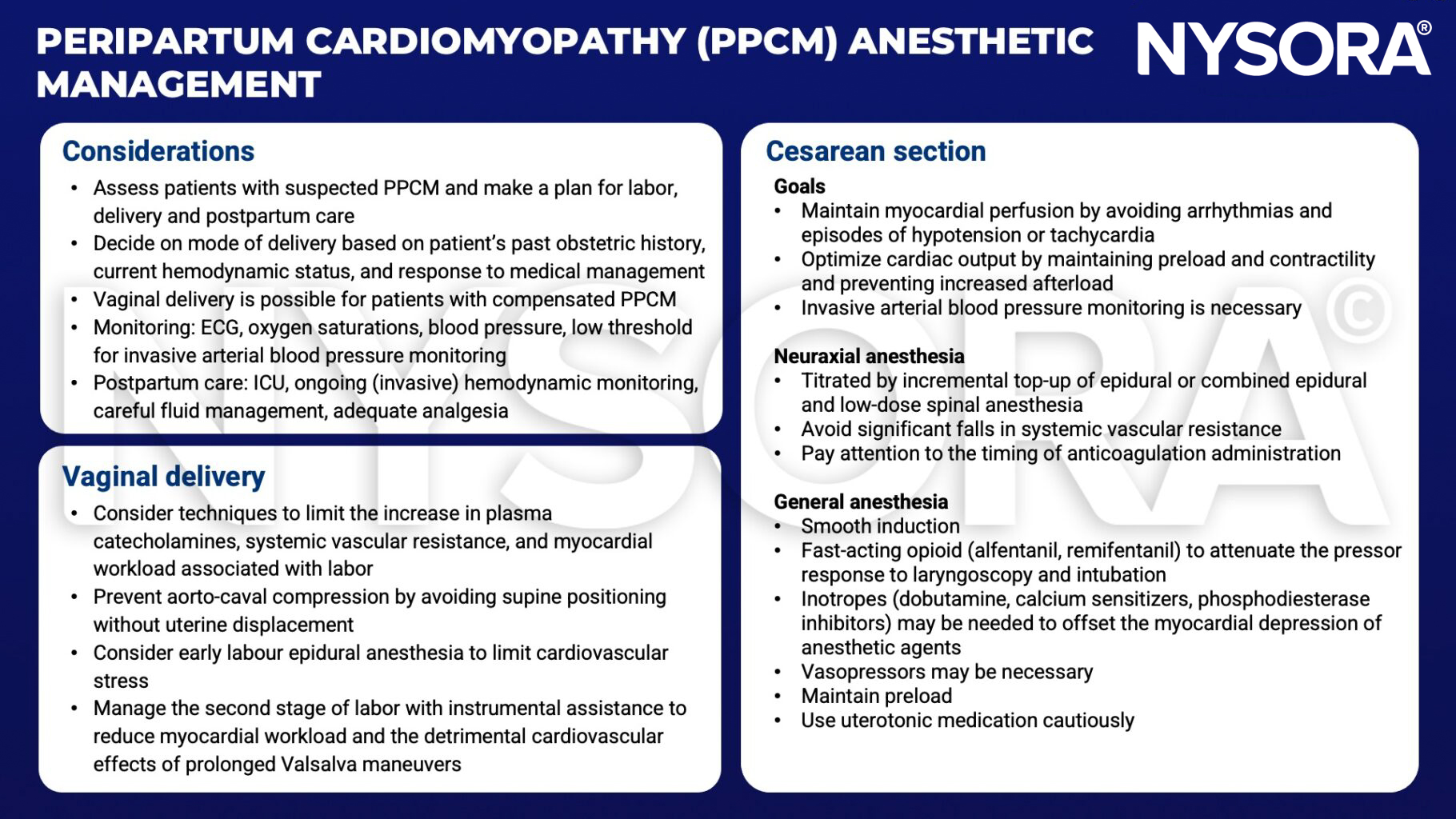
Anesthetic management
Suggested reading
- Rodriguez Ziccardi M, Siddique MS. Peripartum Cardiomyopathy. [Updated 2022 Jul 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482185/
- Honigberg MC, Givertz MM. Peripartum cardiomyopathy. BMJ. 2019;364:k5287. Published 2019 Jan 30. doi:10.1136/bmj.k5287
- Thompson L, Hartsilver E. Peripartum cardiomyopathy. WFSA. https://resources.wfsahq.org/atotw/peripartum-cardiomyopathy/#:~:text=Titrated%20neuraxial%20anaesthesia%2C%20by%20incremental,agents%20that%20reduce%20myocardial%20contractility. Published February 24, 2015. Accessed February 13, 2023.
Clinical updates
Eerdekens et al. (Current Opinion in Anesthesiology, 2023) emphasize that peripartum cardiomyopathy (PPCM) is defined by pregnancy-associated heart failure with LVEF < 45% and is increasingly recognized worldwide, with major advances in understanding its multifactorial pathophysiology involving angiogenic imbalance, inflammation, and genetic susceptibility. The review highlights that management mirrors standard heart failure care but must be adapted to pregnancy status, with beta-blockers, diuretics, hydralazine, digoxin, and LMWH considered safe during pregnancy, while severe cases may require early referral for advanced hemodynamic monitoring and temporary mechanical circulatory support such as ECMO or IABP.