Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Definition and types of Von Willebrand’s Disease (VWD)
- Treatment of VWD
- Anesthetic management of VWD
Definition and mechanisms
- von Willebrand Disease is the most common inherited bleeding disorder with a prevalence of approximately 1% in the population
- Due to a qualitative or quantitative defect of the von Willebrand factor (vWF)
- Three types:
- Type 1 is a quantitative defect
- Type 2 is a qualitative defect
- Type 3 is a very rare but severe form characterized by a mutant inhibitor protein against the vWF (vWF inhibitor)
- It demonstrates autosomal dominant (e.g. type 1, 2B) & – recessive (e.g. types 2M, 2N, 3) inheritance, with marked phenotypic variations
- It may be discovered at any age and in either sex
Signs and symptoms
- Easy bruising
- Recurrent nose bleeds
- Prolonged postoperative or posttraumatic bleeding
- Bleeding gums
- Menorrhagia or in extreme cases even chronic joint bleeding
Complications
- Anemia
- Swelling
- Pain
Acquired von Willebrand Syndrome
- Is extremely rare but has been documented in clonal hematological, cardiovascular (aortic valve stenosis with higher sheer stresses in the vessels), and immunological (hypothyroidism), and other lymphoproliferative auto-immune diseases
- A vWF-inhibitor protein or the adhesion of vWF with malignant cells can occur
- It has a marked reduced vWF activity interfering with the production and/or the stability of vWF
- Leading to the production of autoantibodies to endogenous vWF which can result in decreased functional high molecular weight vWF multimers
- Acquired vWS responds well to vWF-concentrates administration but the effects can be mitigated by these inhibitor proteins since they affect the half-life time of the administered vWF
von Willebrand factor
- vWF is a ligand between platelets and subendothelial cells
- vWF stabilizes circulating factor VIII hereby preventing its degradation
- On average the levels of vWF and FVIII are lower in humans with type O blood and are increased in inflammatory conditions and during pregnancy
- Bleeding time and platelet function analysis will be prolonged in relation to the severity of the abnormality
- APTT can be prolonged in relation to the remaining quantity of FVIII
Diagnosis
- Laboratory testing: VWF-antigen, VWF-activity, and FVIII
- Familial history
Types
Determination of the exact type is of utmost importance for the therapeutical approach
| Type 1 | Type 2 | Type 3 |
|---|---|---|
| ~85% with vWD have this form Decreased quantities of vWF in several degrees Characterized by a mild bleeding tendency but has increased risks peri-operatively Responds well to desmopressin infusion | ~ 5% with vWD have this form Subtypes 2A, 2B, 2M, and 2N are described Types 2A and 2B differ in the platelet binding capacity but the amount of high molecular weight multimers circulating in the plasma is decreased in both Type 2A presents with a decreased platelet binding Type 2B presents with an increased platelet agglutination with a concomitant increased risk of thrombosis Type 2B is marked by accompanying thrombocytopenia due to a higher clearance of platelets Subtype 2M has a decreased platelet binding with normal quantities of HMW multimers Subtype 2N is characterized by a flawed ability to stabilize circulating FVIII and results in a factor VIII deficiency | A complete defect in vWF synthesis Plasma factor VIII is decreased despite normal synthesis due to the lack of stabilization by the total absence of vWF |
Major bleeding risks
- Need to be considered when FVIII < 30IU/dL & Thrombocytopenia < 50000/mm³
Treatment

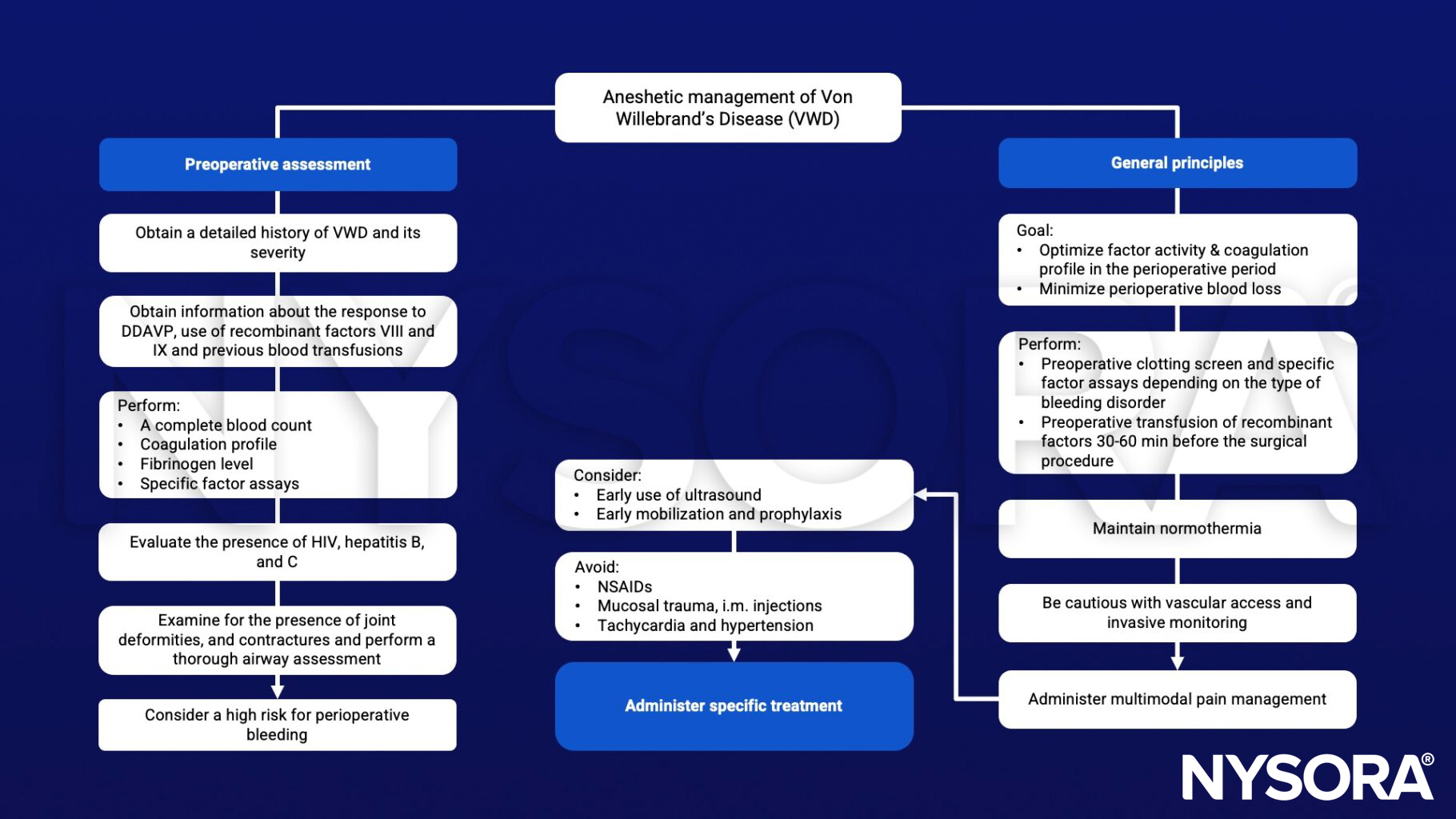
Anesthetic management
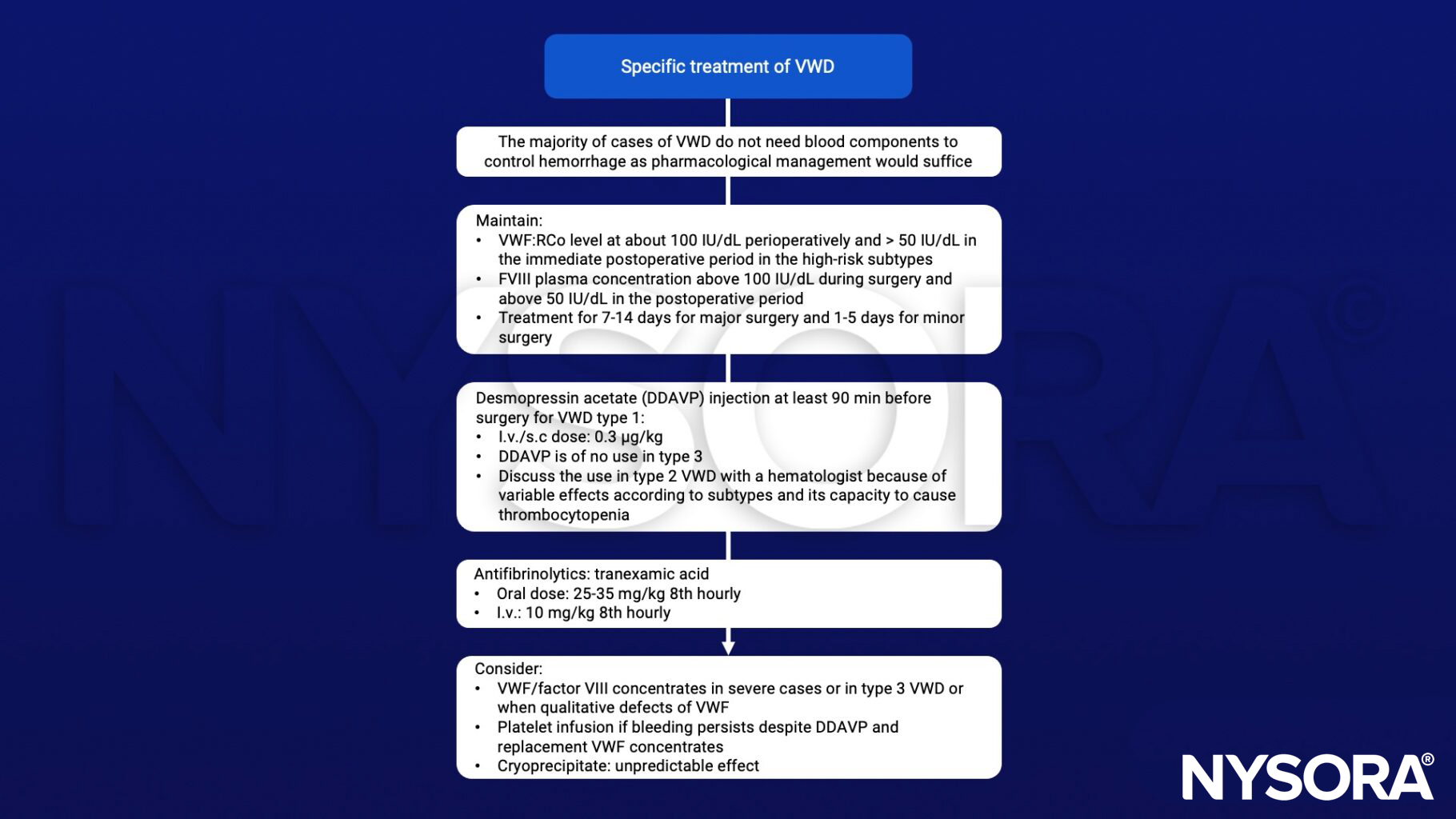
Specific treatment during anesthesia
Suggested reading
- Uptodate: von Willebrand disease (vWD):Treatment of major bleeding and major surgery, Paula James, MD, FRCPC, literature review current Nov 2022, last updated Sep 12, 2022.
- Shah UJ, Madan Narayanan M, J Graham Smith JH. Anaesthetic considerations in patients with inherited disorders of coagulation. Continuing Education in Anaesthesia Critical Care & Pain, Volume 15, Issue 1, February 2015, Pages 26–31.
- Training in anaesthesia: the essential curriculum; Oxford Specialty Training, Chapter 15 pp392-393; ISBN: 978-0-19-922726-6