
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the physiological changes associated with pregnancy and their anesthetic implications
- Describe the anesthetic implications of commonly used medications
- Manage obstetric patients presenting for non-obstetric surgery
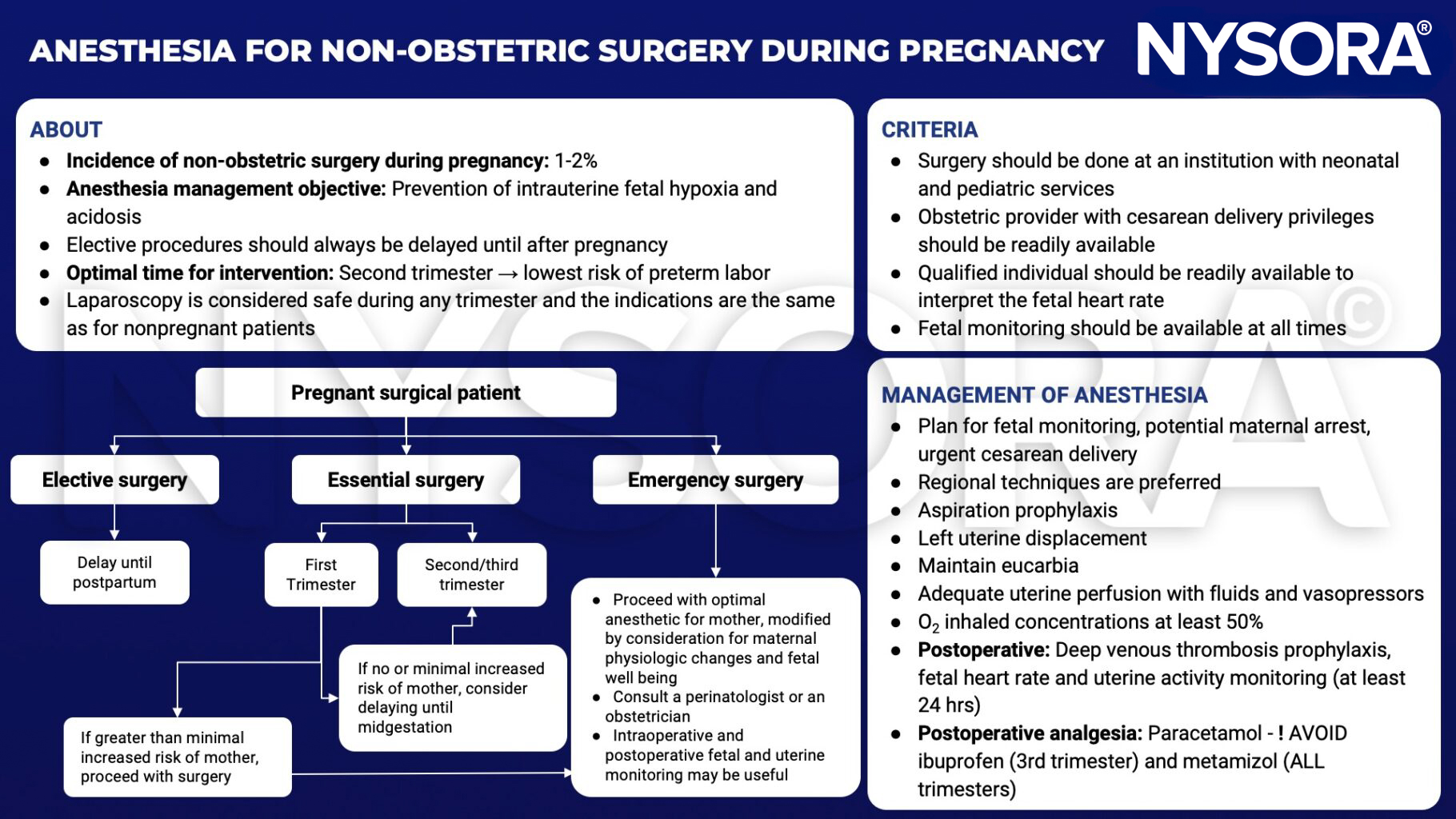
Background
- Non-obstetric surgery may be required at any trimester during pregnancy, which carries the unique challenge of caring simultaneously for two patients
- Understanding the physiological changes of pregnancy is essential for safe anesthesia
- Most common indications: Acute appendicitis, cholecystitis, trauma, and surgery for maternal malignancies
- Main risks: Fetal loss, premature labor, and delivery
Physiological changes & implications
| System | Physiological change | anesthetic implications |
|---|---|---|
| Cardiovascular | Increased cardiac output by up to 50% Increased uterine perfusion up to 10% of cardiac output Decreased systemic vascular resistance, pulmonary vascular resistance, and arterial pressure Aortocaval compression from 13 weeks | Uterine perfusion not autoregulated Hypotension common under regional and general anesthesia Supine hypotensive syndrome requires left lateral tilt |
| Respiratory | Increased minute ventilation Respiratory alkalosis Decreased expiratory reserve volume, residual volume, and functional residual capacity Ventilation/perfusion mismatch Increased oxygen consumption Upward displacement of diaphragm Increased thoracic diameter Mucosal edema | Potential hypoxemia in the supine and Trendelenburg positions Breathing more diaphragmatic than thoracic Difficult laryngoscopy and intubation; bleeding during attempts |
| Central nervous system | Epidural vein engorgement Decreased epidural space volume Increased sensitivity to opioids and sedatives | More extensive local anesthetic spread |
| Hematological | 30% red cell volume increase Increased white blood cell count 50% plasma volume increase Increased coagulation factors Decreased albumin and colloid osmotic pressure | Dilutional anemia Thromboembolic complications Edema, decreased protein binding of drugs |
| Gastrointestinal | Increased intragastric pressure Decreased barrier pressure | Increased aspiration risk Antacid prophylaxis, RSI after 18 weeks gestation |
| Renal | Increased renal plasma flow and glomerular filtration rate Decreased reabsorptive capacity | Normal urea and creatinine may mask impaired renal function Glycosuria and proteinuria |
Medication side-effects & anesthetic implications
| Medication | Side-effects and anesthetic implications |
|---|---|
| Volatile agents | Decreased MAC, reduced uterine tone, hypotension |
| Nitrous oxide | Prolonged exposure may inhibit DNA synthesis; avoid in the first trimester |
| Succinylcholine | Reduced plasma cholinesterase, possible prolonged action |
| Non-depolarizing neuromuscular blocking agents | Quaternary ammonium compounds do not cross the placenta |
| Local anaesthetics | Reduced protein-binding, increased risk of toxicity; use lower intrathecal doses in late pregnancy |
| Opioids | Increased maternal sensitivity, fetal withdrawal, intrauterine growth restriction with chronic use |
| Non-steroidal anti-inflammatory drugs | Premature ductus arteriosus closure, avoid after 28 weeks; ketorolac contraindicated |
| Warfarin | Teratogenic, crosses the placenta |
| Heparin | Does not cross the placenta |
| Atropine | Fetal tachycardia, crosses the placenta |
| Glycopyrrolate | Quaternary ammonium compound, does not cross the placenta |
| Phenytoin, carbamazepine, sodium valproate | Congenital malformations (neural tube defects) |
| Magnesium sulphate | Muscle weakness, interaction with neuromuscular blocking agents |
| ACE inhibitors | Intrauterine growth restriction, oligohydramnios, renal impairment |
| Beta-blockers | Intrauterine growth restriction, neonatal hypoglycemia, bradycardia |
| Thiazides | Neonatal thrombocytopenia |
| Beta-2-agonists: ritodrine, terbutaline, salbutamol | Tachyarrhythmias, pulmonary edema, hypokalemia, hyperglycemia |
| Oxytocin receptor antagonists: atosiban | Nausea, vomiting, fewer side-effects than beta-2-agonists |
| Calcium-channel blockers: nifedipine | Hypotension, fewer side-effects than beta-2-agonists |
Management
Suggested reading
- Haggerty E, Daly J. Anaesthesia and non-obstetric surgery in pregnancy. BJA Education. 2021;21(2):42-3.
- Nejdlova M, Johnson T. Anaesthesia for non-obstetric procedures during pregnancy. Continuing Education in Anaesthesia Critical Care & Pain. 2012;12(4):203-6.











