Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About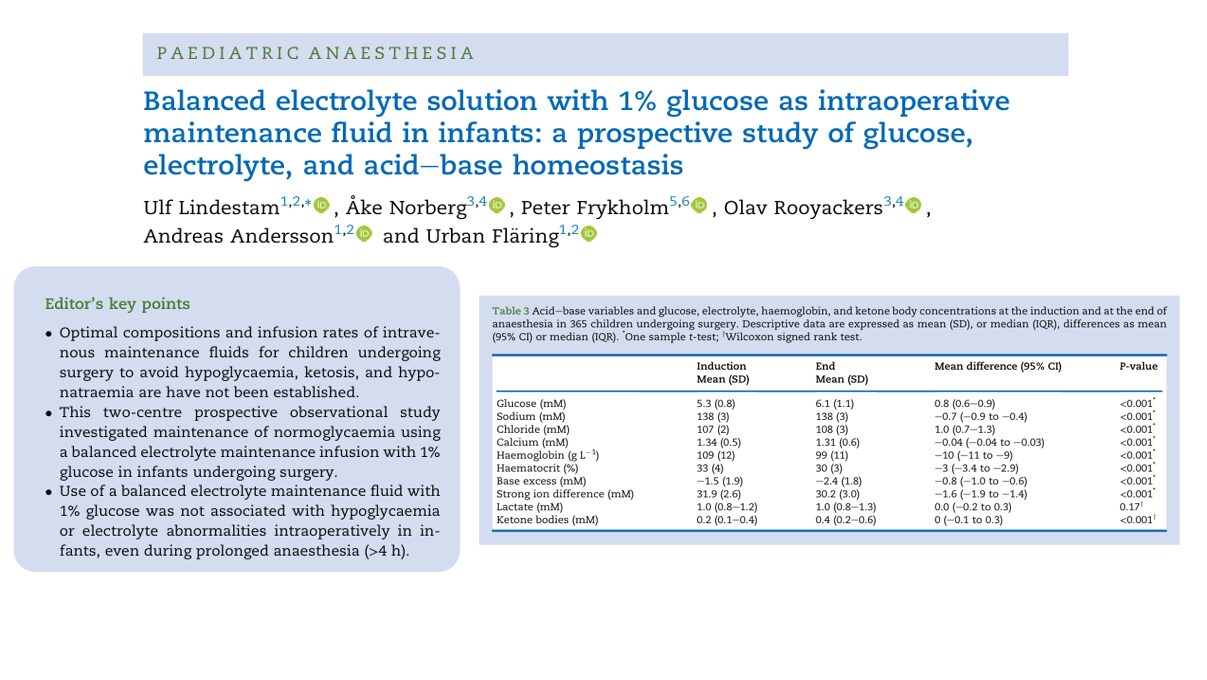





Ensuring safe and effective fluid management in infants undergoing surgery is a critical concern in pediatric anesthesia. Balancing the risks of hypoglycemia, hyponatremia, and metabolic instability has long presented a challenge. A landmark prospective study published in the British Journal of Anaesthesia offers robust evidence that a balanced electrolyte solution containing 1% glucose is both effective and safe for intraoperative maintenance in infants.
Why this matters
Infants, due to their unique physiology, are particularly susceptible to intraoperative metabolic derangements:
- High basal metabolic rate
- Limited glycogen reserves
- Immature endocrine response
- Increased sensitivity to fluid shifts
Historically, concerns about hypoglycemia led to the liberal use of glucose-rich, often hypotonic, intravenous (IV) solutions. However, these practices introduced other risks, particularly hyponatremia and hyperglycemia, prompting a reevaluation of intraoperative fluid protocols.
The study at a glance
Conducted at two major Swedish centers – Karolinska University Hospital in Stockholm and Uppsala University Hospital – this large prospective observational study included 365 infants aged 1–12 months. All underwent surgery under general anesthesia with standardized administration of a 1% glucose-balanced electrolyte solution (Benelyte, Fresenius Kabi).
- Primary goal: Determine the incidence of intraoperative hypoglycemia.
- Secondary goals: Evaluate glucose, electrolyte, ketone, and acid-base balance.
Key characteristics:
- Age range: 1–12 months (mean 5.2 months)
- Exclusions: Prematurity <44 weeks PCA, metabolic disease, hepatic impairment
- Infusion rates: 3.97 mL/kg/h median (range: 4–8 mL/kg/h)
- Monitoring: Glucose every 30–60 minutes, full blood analysis pre- and post-anesthesia
Main findings
- No cases of hypoglycemia
- Mean plasma glucose rose from 5.3 to 6.1 mM (p<0.001)
- No infant recorded glucose <3.0 mM
- Even among the youngest infants (≤3 months), levels remained stable or improved
- Mild hyperglycemia (>8.3 mM) was rare (4.3% of patients)
This result supports that 1% glucose is sufficient to maintain normoglycemia even with modest infusion rates and prolonged fasting.
- Sodium and chloride stayed within safe limits
- Mean sodium dropped slightly: 138 to 137.3 mM (p<0.001)
- Hyponatremia (<135 mM) rose slightly from 3.6% to 6.6%—but remained clinically insignificant
- Chloride increased from 107 to 108 mM, with 13.2% showing mild hyperchloremia at the surgery end
Infants receiving albumin boluses showed smaller sodium reductions, possibly due to their hypertonic properties.
- Acid-base and ketone trends remained mild
- Base excess (BE) declined from −1.5 to −2.4 mM, within a safe range
- Ketone levels increased modestly, particularly in surgeries >180 minutes
- No cases of dangerous acidosis or ketosis were recorded
Ketosis, a marker of fasting stress, remained largely within acceptable thresholds.
- Fasting did not significantly impact stability
Although 21% of infants fasted >6 hours, no association was found with adverse glucose or ketone trends.
- Median breastmilk/formula fast: 5 hours
- Only 12.3% received glucose-containing clear fluids pre-op
This suggests that adherence to updated fasting guidelines (6-4-1 rule) is generally safe when paired with appropriate fluid management.

Clinical implications
This study offers the strongest evidence to date supporting the intraoperative use of 1% glucose-balanced electrolyte fluids in infants. Its findings could lead to practice changes, including:
- Standardizing low-glucose, isotonic solutions in pediatric ORs
- Reducing unnecessary glucose supplementation
- Preventing avoidable complications such as cerebral edema from hyponatremia or hyperglycemia-induced immune impairment
Benefits of 1% glucose-balanced fluids
- Maintains metabolic and electrolyte stability
- Reduces risk of glucose and sodium disturbances
- Matches modern anesthetic practices (regional blocks, reduced fasting)
Step-by-step clinical protocol
- Pre-op screening
- Rule out metabolic or endocrine disease
- Confirm normal liver/kidney function
- Fasting prep
- Breastmilk: 4–6 hours
- Clear fluids: up to 1 hour pre-op
- Start infusion
- 4–8 mL/kg/h using 1% glucose-balanced solution
- Initial rate may be higher (10 mL/kg/h) to compensate for fasting
- Intraoperative monitoring
- Glucose: baseline, every 30–60 minutes
- Electrolytes and acid-base: at least at induction and end
- Adjust fluids or add boluses as needed
- Post-op reassessment
- Check glucose and sodium before full recovery
- Consider continued isotonic fluids if extended fasting is expected
Recommendations
For hospitals and anesthetists:
- Adopt balanced isotonic solutions with 1% glucose as standard for infants
- Train staff in correct dosing and monitoring protocols
- Phase out hypotonic high-glucose fluids to minimize sodium-related risks
For researchers:
- Investigate optimal fluid choices in special populations (preterms, neonates, endocrine disorders)
- Explore longer-term effects on recovery and neurological outcomes
Final thoughts
This comprehensive prospective study underscores a pivotal shift in pediatric anesthesia toward safer, smarter fluid choices tailored to the unique metabolic demands of infants. With compelling evidence that 1% glucose-balanced electrolyte solutions effectively safeguard against intraoperative hypoglycemia and electrolyte imbalance, clinicians have a validated, evidence-backed foundation for updating protocols.
For more detailed information, refer to the full article in British Journal of Anaesthesia
Reference: Lindestam U, Norberg Å, Frykholm P, Rooyackers O, Andersson A, Fläring U. Balanced electrolyte solution with 1% glucose as intraoperative maintenance fluid in infants. Response to Br J Anaesth 2025; 135: 798-9. Br J Anaesth.
For more literature updates in pediatric anesthesia, read NYSORA’s Pediatric Anesthesia Updates 2025!