Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Define and classify aortic dissection
- Describe the risk factors for aortic dissection
- Diagnose aortic dissection
- Manage patients with aortic dissection
Definition & mechanisms
- Life-threatening emergency
- Most common type of acute aortic syndrome
- Occurs when a tear in the aortic intima allows blood to dissect into the wall of the aorta
- Can result from abnormalities in underlying tissue structure (Marfan syndrome, Loeys-Dietz syndrome)
- Can also occur in previously asymptomatic patients with no known genetic aortopathy
- Often associated with an increase in physical activity or stress, leading to acute hypertension
Classification
There are several classification systems for aortic dissection:
| DeBakey | Type I | Tear in the ascending portion; involves all portions of the thoracic aorta |
| Type II | Tear in the ascending aorta; involves the ascending aorta only, stopping before the innominate artery |
|
| Type III | Tear located in the descending segment; almost always involves the descending thoracic aorta only, starting distal to the left subclavian artery; can propagate proximally into the arch |
|
| Stanford | Type A | All dissections involving the ascending aorta irrespective of the site of tear |
| Type B | All dissections that do not involve the ascending aorta |
Risk factors
| Lifestyle factors | Long-term arterial hypertension | |
| Smoking | ||
| Dyslipidemia | ||
| Cocaine, crack cocaine, or amphetamine use | ||
| Connective tissue disorders | Marfan’s syndrome | |
| Loeys-Dietz’s syndrome | ||
| Ehlers-Danlos syndrome | ||
| Turner’s syndrome | ||
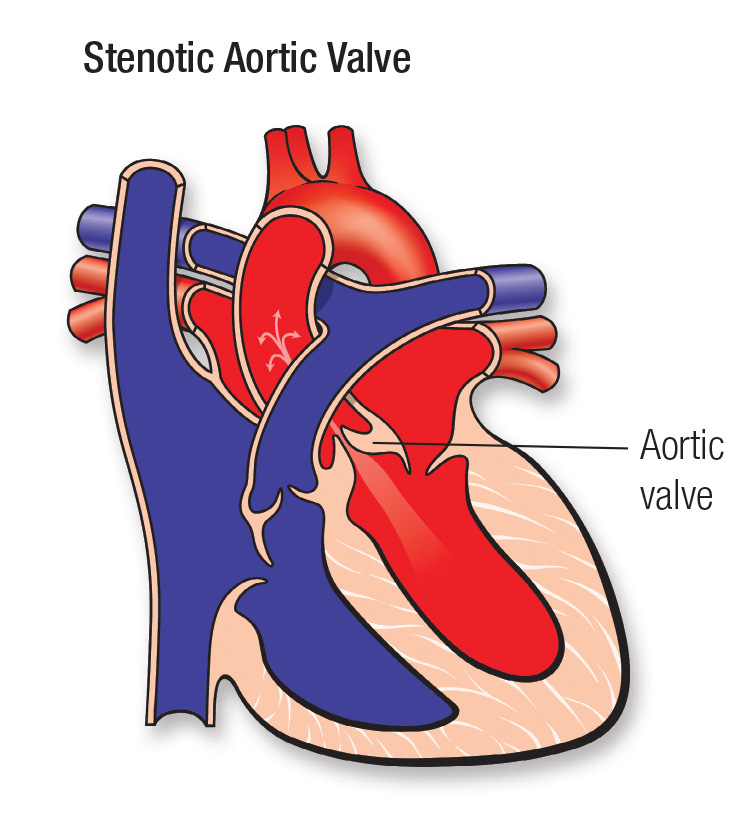
| Hereditary vascular disease | Bicuspid aortic valve | |
| Coarctation of the aorta | ||
| Vascular inflammation | Autoimmune disorders | Giant-cell arteritis |
| Takayasu’s arteritis | ||
| BehÇet’s disease |
||
| Ormond’s disease | ||
| Infection | Syphilis | |
| Tuberculosis | ||
| Deceleration trauma | Car accident | |
| Iatrogenic factors | Catheter or instrument intervention | |
| Valvular or aortic surgery | Side-clamping, cross-clamping, or aortotomy | |
| Graft anastomosis | ||
| Patch aortoplasty |
Diagnosis
- Imaging
- CT
- The triple rule-out protocol is the one-stop CT examination for chest pain designed to differentiate acute coronary syndrome, pulmonary embolism, and acute aortic dissection
- Transthoracic echocardiography (TTE)
- Transesophageal echocardiography (TEE)
- More complete imaging of the aorta than TTE
- MRI
- Can combine anatomical and functional information in one examination and provide a comprehensive evaluation of aortic dissection
- CT
- Biomarkers
- D-dimer and fibrin degradation products
- Smooth muscle myosin heavy chain
- Matrix metalloproteinase-9
- Elastin degradation products
- Calponin
- Transforming growth factor-beta (TGFβ)
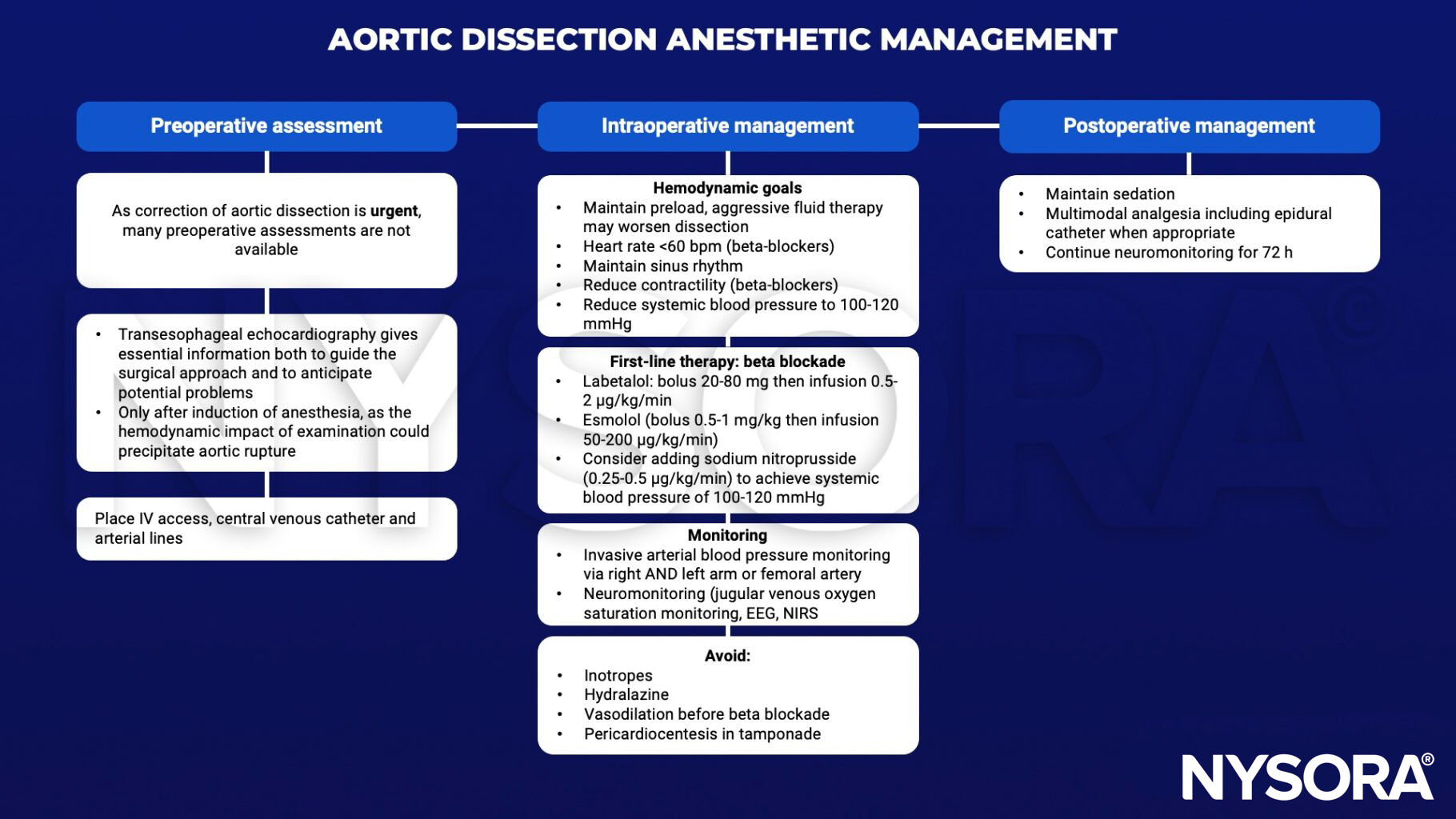
Management
Suggested reading
- Agarwal S, Kendall J, Quarterman C. Perioperative management of thoracic and thoracoabdominal aneurysms. BJA Educ. 2019;19(4):119-125.
- Gregory SH, Yalamuri SM, Bishawi M, Swaminathan M. The Perioperative Management of Ascending Aortic Dissection. Anesth Analg. 2018;127(6):1302-1313.
- Nienaber CA, Clough RE. Management of acute aortic dissection. Lancet. 2015;385(9970):800-811. doi:10.1016/S0140-6736(14)61005-9
Clinical updates
Meacham KS et al. (British Journal of Anaesthesia, 2025) report in a systematic review of 50 studies that most IV antihypertensives used for hypertensive emergencies, such as labetalol, nicardipine, clevidipine, and metoprolol, do not significantly reduce cerebral blood flow (CBF), whereas nitroprusside and nitroglycerin were associated with a median 14% CBF reduction in awake normotensive patients. These findings are highly relevant to acute aortic dissection, where rapid blood pressure reduction is lifesaving but excessive or poorly selected therapy may risk cerebral hypoperfusion.
- Read more about this study HERE.