Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe antiphospholipid antibody syndrome (APS)
- Signs and symptoms and management of APS
Definition and mechanism
- Antiphospholipid syndrome (APS) or Hughes syndrome is a disorder of the immune system that creates antibodies that attack tissues in the body by mistake
- These antibodies can cause blood clots to form in arteries and veins, leading to a heart attack, stroke, and other conditions
- Can result in miscarriage and stillbirth during pregnancy
- Primary APS: the sole manifestation of an autoimmune process
- Secondary APS: in association with another disease such as systemic lupus erythematosus
- Antiphospholipid syndrome is more common in women than in men
- Causes are not completely understood and include environmental or genetic factors or an existing autoimmune disorder
- In very rare cases, blood clots can suddenly form throughout the body, resulting in multiple organ failures → catastrophic antiphospholipid syndrome (CAPS), or Asherson syndrome
- CAPS requires immediate emergency treatment with high-dose anticoagulants
Signs and symptoms
| Vascular thrombosis | Arterial thrombosis | Stroke Transient ischaemic attack Myocardial infarction Venous thrombosis |
| Venous thromboembolism | Venous thromboembolism Pulmonary embolism Small vessel thrombosis |
|
| Obstetric morbidity | ≥ 1 unexplained fetal death at or beyond week 10 of gestation ≥ 1 premature birth due to severe pre-eclampsia, eclampsia, or consequences of placental insufficiency ≥ 3 unexplained consecutive spontaneous abortions before week 10 of gestation | |
| Cardiac manifestations | Valvular heart disease Cardiomyopathies | |
| Neurological manifestations | Cognitive dysfunction Headache or migraine Multiple sclerosis Transverse myelopathy Epilepsy | |
| Dermatologic manifestations | Livedo reticularis Skin ulceration Pseudo-vasculitic lesion Distal gangrene Superficial phlebitis Malignant atrophic papulosis-like lesion Subungual splinter hemorrhage | |
| Renal manifestations | Thrombotic microangiopathy Chronic vascular damage | |
| Hematologic manifestations | Thrombocytopenia Hemolytic anemia |
Risk factors
- Pregnancy
- Immobility
- Surgery
- Smoking
- Oral contraceptives or estrogen therapy for menopause
- High cholesterol and triglyceride levels
- Systemic autoimmune diseases such as lupus
Complications
- Kidney failure
- Stroke
- Cardiovascular problems
- Pulmonary embolism
- Pregnancy complications
- Miscarriages
- Stillbirths
- Premature delivery
- Slow fetal growth
- Pre-eclampsia
Treatment
- Primary thromboprophylaxis for aPL carriers with no prior history of vascular thrombosis and/or obstetric events
- Low-dose aspirin (75-100 mg/d)
- Lifestyle changes: smoking cessation, weight loss, control of hypertension and hyperlipidemia
- A prophylactic dose of low-molecular-weight heparin (LMWH) in high-risk situations such as surgery, prolonged immobilization, and the puerperium
- Secondary thromboprophylaxis for the prevention of recurrence after thrombotic and/or obstetric events in patients with a prior history
- Previous venous thrombosis:
- Anticoagulation: target INR of 2.0-3.0
- Previous arterial thrombosis:
- High-intensity anticoagulation: target INR of 3.0-4.0 or a target INR of 2.0–3.0 combined with low-dose aspirin
- Previous venous thrombosis:
- CAPS
- Combination therapy with glucocorticoid, heparin, and plasmapheresis or IV immunoglobulin, rituximab, cyclophosphamide, or eculizumab
- Pregnant women
- Combination therapy:
- Low-dose aspirin and unfractionated heparin or LMWH
- Withdraw oral anticoagulants as soon as pregnancy is confirmed to prevent teratogenicity
- Patients without a history of thrombosis:
- Low-dose aspirin and a prophylactic dose of unfractionated heparin or LMWH are used for primary prevention
- Patients with a history of thrombotic events:
- Low-dose aspirin and a prophylactic dose of unfractionated heparin or LMWH are used for secondary prevention
- After delivery:
- Administer a prophylactic dose of LMWH for at least 6 weeks after delivery
- Start warfarin as soon as possible after bleeding is controlled
- Patients with APS who have not received any thromboprophylaxis before delivery and do not carry any risk factors for thrombosis, require LMWH for only 7 days following delivery
- Combination therapy:
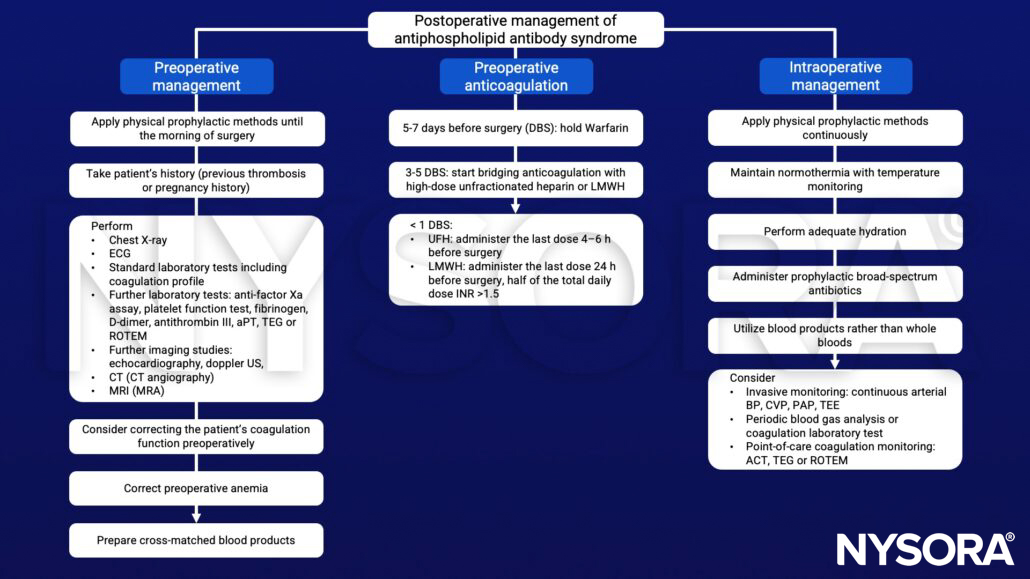
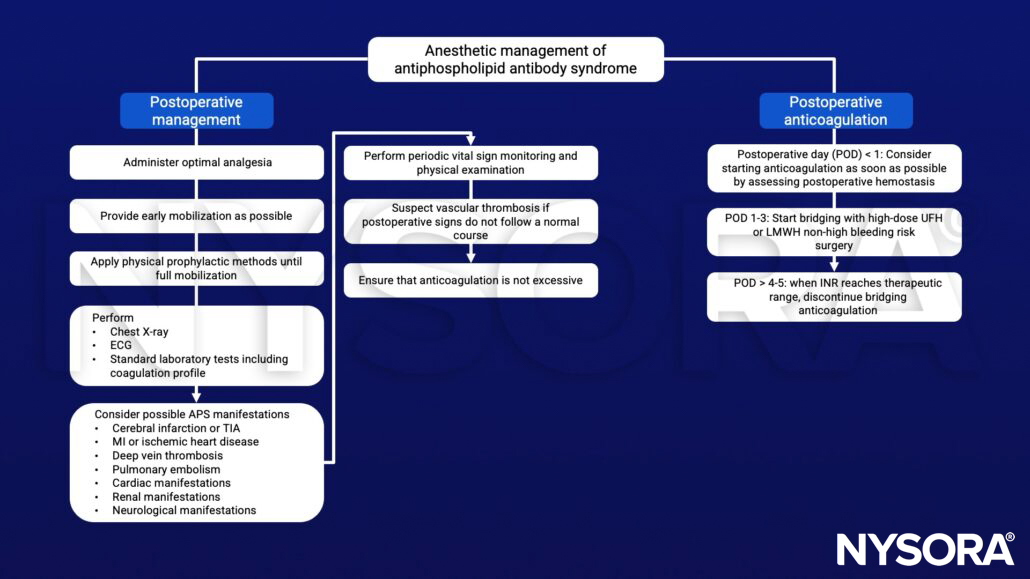
Management
Suggested reading
- Kim JW, Kim TW, Ryu KH, Park SG, Jeong CY, Park DH. Anaesthetic considerations for patients with antiphospholipid syndrome undergoing non-cardiac surgery. J Int Med Res. 2020;48(1):300060519896889.