Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Background of videolaryngoscopy
- Advantages and disadvantages of videolaryngoscopy
Background
- Videolaryngoscopy utilizes video camera technology to visualize airway structures and facilitate endotracheal intubation
- Videolaryngoscopy is an alternative to direct laryngoscopy for airway intubation in adults and children as it improves airway safety and is associated with fewer failed attempts and complications
- Is also a new diagnostic and therapeutic tool in head and neck surgery
- Has the great advantage of reducing difficult views of the laryngeal opening (glottis)
- Despite a good view of the cords, difficulty may be encountered in advancing the tube through the glottis with videolaryngoscopy
- Use the mnemonic aid “CCL” to prepare for videolaryngoscopy:
- Choose the right tube
- Check the endotracheal tube cuff
- Lubricate the stylet and the endotracheal tube
- Load the stylet (band it according to the angle of the videolaryngoscopy blade)
- Consider the possibility of airway trauma during videolaryngoscopy as the operator’s attention is diverted from the direct view of the proximal airway to the indirect view of the glottis on the monitor
- Therefore, introduce the tip of the tube and stylet into the oropharynx under direct vision and then advance as guided by the indirect view on the monitor
Indications and contraindications
- Indications
- Hypoxia or hypoventilation requiring assisted ventilation to maintain oxygenation and ventilation
- Apnea or impending respiratory arrest
- Elective anesthesia
- Need for prolonged mechanical ventilation
- Situations where bag-valve-mask ventilation is difficult or impossible or upper airway obstruction due to soft tissues
- Need to prevent aspiration (eg, in obtunded or comatose patients) or for repeated airway suction
- Contraindications
- Absolute:
- Restricted mouth opening that blocks tube insertion
- Impassable upper airway obstruction
- Relative:
- Blood or emesis in the airway
- Foreign body removal
- Consciousness or presence of a gag reflex
- Absolute:
Complications
- Palatal perforation
- Palatopharyngeal arch tear
- Injury to tonsilar pillars
- Dental or oropharyngeal soft tissue trauma during tube insertion
- Vomiting and aspiration during tube insertion
- Incorrect tube placement (eg, esophageal intubation)
- Hypoxia during the intubation attempt
Clinical usage
- Orotrachelal intubation
- Nasotracheal intubation
- Intubation of cervical spine pathology
- Awake intubation
- Conduit for flexible fiberoptic bronchoscope
- Insertion of different devices into the oropharynx
- Diagnosis and recording of upper airway pathology
Advantages and disadvantages
Advantages Disadvantages
Easier to learn and maintain the skill (by observing the video screen)
Effective tool for those who infrequently intubate as well as students learning to intubateSucces rate is not 100%
Less workforce is needed to view the glottis
Improved glottic visualizationUnknown efficacy in routine airway management and the efficacy of different videolaryngoscopes differs
A higher first-pass success rate of tracheal intubation in patients with difficult airways versus direct laryngoscopy and thus a lower incidence of multiple attemts
A higher incidence of oropharyngeal injury
Superior view of the glottic opening versus direct laryngoscopy Prolonged intabution time due to difficult tracheal tube delivery into the glottic opening
A lower incidence of inadvertent esophageal intubation versus direct laryngoscopy The camera view can frequently be blurred by foging, secretions, blood, or emesis in the oropharynx
Easier to confirm pathological changes (laryngeal edema) after repeated attempts at trachel intubation Two-dimensional view with loss of depth perception
It is not necessary to align airway axes (oral-pharyngeal-laryngeal) to achieve line of sight More expensive and still not widely available
Less cervical manipulation Potential weakening in development/maintenance of direct laryngoscopy skill set
Possible awake assessment/intubation Potential for false sense of security and lack of preparation for a difficult airway
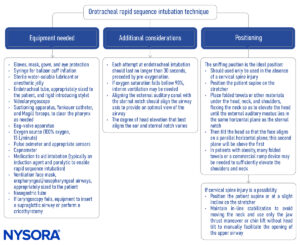
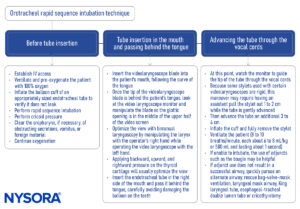
Orotracheal intubation technique
Suggested reading
- Asai T, Jagannathan N. Videolaryngoscopy Is Extremely Valuable, But Should It Be the Standard for Tracheal Intubation?. Anesth Analg. 2023;136(4):679-682.
- Prekker ME, Driver BE, Trent SA, et al. Video versus Direct Laryngoscopy for Tracheal Intubation of Critically Ill Adults [published online ahead of print, 2023 Jun 16]. N Engl J Med. 2023;10.1056/NEJMoa2301601.
- Hansel, J., Rogers, A.M., Lewis, S.R., Cook, T.M., Smith, A.F., 2022. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation: a Cochrane systematic review and meta-analysis update. British Journal of Anaesthesia 129, 612–623.
- Goranović, T., 2021. Videolaryngoscopy, the Current Role in Airway Management. https://doi.org/10.5772/intechopen.93490
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Chemsian R, Bhananker S, Ramaiah R. Videolaryngoscopy. Int J Crit Illn Inj Sci. 2014;4(1):35-41.
Clinical updates
Ahmad et al. (BJA, 2025) reinforce videolaryngoscopy as a central tool in managing unanticipated difficult tracheal intubation, with the Difficult Airway Society now strongly emphasizing its use to maximize first-pass success. The updated DAS algorithm integrates videolaryngoscopy early in Plan A, reflecting evidence that it improves glottic visualization and reduces failed intubation and complication rates compared with direct laryngoscopy.
Kristensen et al. (Current Opinion in Anesthesiology, 2025) emphasize that head and neck surgery represents a uniquely high-risk airway population in which awake tracheal intubation, videolaryngoscopy, and flexible bronchoscopy are central to preventing loss of airway control. The review highlights videolaryngoscopy as a key first-line or adjunctive tool that improves glottic visualization and first-pass success despite distorted anatomy, while reinforcing the need for clear backup strategies, including supraglottic devices and early front-of-neck access.
- Read more about this study HERE.
Gómez-Ríos et al. (EJA, 2025) recommend routine use of videolaryngoscopy (VL) as the primary device for tracheal intubation, based on evidence that it improves first-attempt success and reduces complications such as oesophageal intubation and airway trauma compared with direct laryngoscopy. The guideline proposes 12 consensus recommendations to enable universal VL adoption, including ensuring device availability in all airway management areas, integrating VL into clinical guidelines and algorithms, and incorporating high-fidelity simulation training.