
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the overall mechanisms and common causes of status epilepticus
- Describe the signs of status epilepticus
- Prevent status epilepticus
- Manage status epilepticus
Definition & mechanisms
- Status epilepticus is defined as more than 30 minutes of either 1) continuous seizure activity or 2) two or more sequential seizures without full recovery of consciousness between seizures
- Cerebral damage is more likely if the seizure is prolonged
- There are lots of different types of seizures and not all of them involve obvious convulsive activity
- Epilepsy can occur at any age but is commonly diagnosed in those aged below 20 or over 65 years
- First stage is characterized by an increase in:
- Cerebral metabolism
- Blood flow
- Glucose and lactate concentration
- Compensatory mechanisms:
- Massive catecholamine release
- Raised cardiac output
- Hypertension
- Increased central venous pressure
- After 30-60 min, compensatory mechanisms fail:
- Hypoxia
- Hypoglycemia
- Increased intracranial pressure
- Cerebral edema
- Hyponatremia
- Potassium imbalance
- Evolving metabolic acidosis
- Consumptive coagulopathy
- Rhabdomyolysis
- Multi-organ failure
Etiology
- Acute
- Stroke
- Metabolic abnormalities
- Hypoxia
- Systemic infection
- Anoxia
- Trauma
- Traumatic brain injury
- Drug overdose
- CNS infection
- CNS hemorrhage
- Chronic
Signs & symptoms
Status epilepticus can present in several forms:
- Convulsive: unresponsiveness and tonic, clonic, or tonic-clonic movements of the extremities
- Non-convulsive: prolonged seizure activity evidenced by epileptiform discharges on EEG, change in behavior or cognition in some patients
- Electrographic: commonly used for comatose patients who show electrographic evidence of prolonged seizure activity
Diagnosis
- Based on history and clinical examination
- Often present either actively convulsing or minimal time between clustered seizures
Prevention
- Seizure detection based on EEG and immediate treatment
- In patients with a history of well-controlled epilepsy, avoid disruption of antiepileptic medication perioperatively
Management
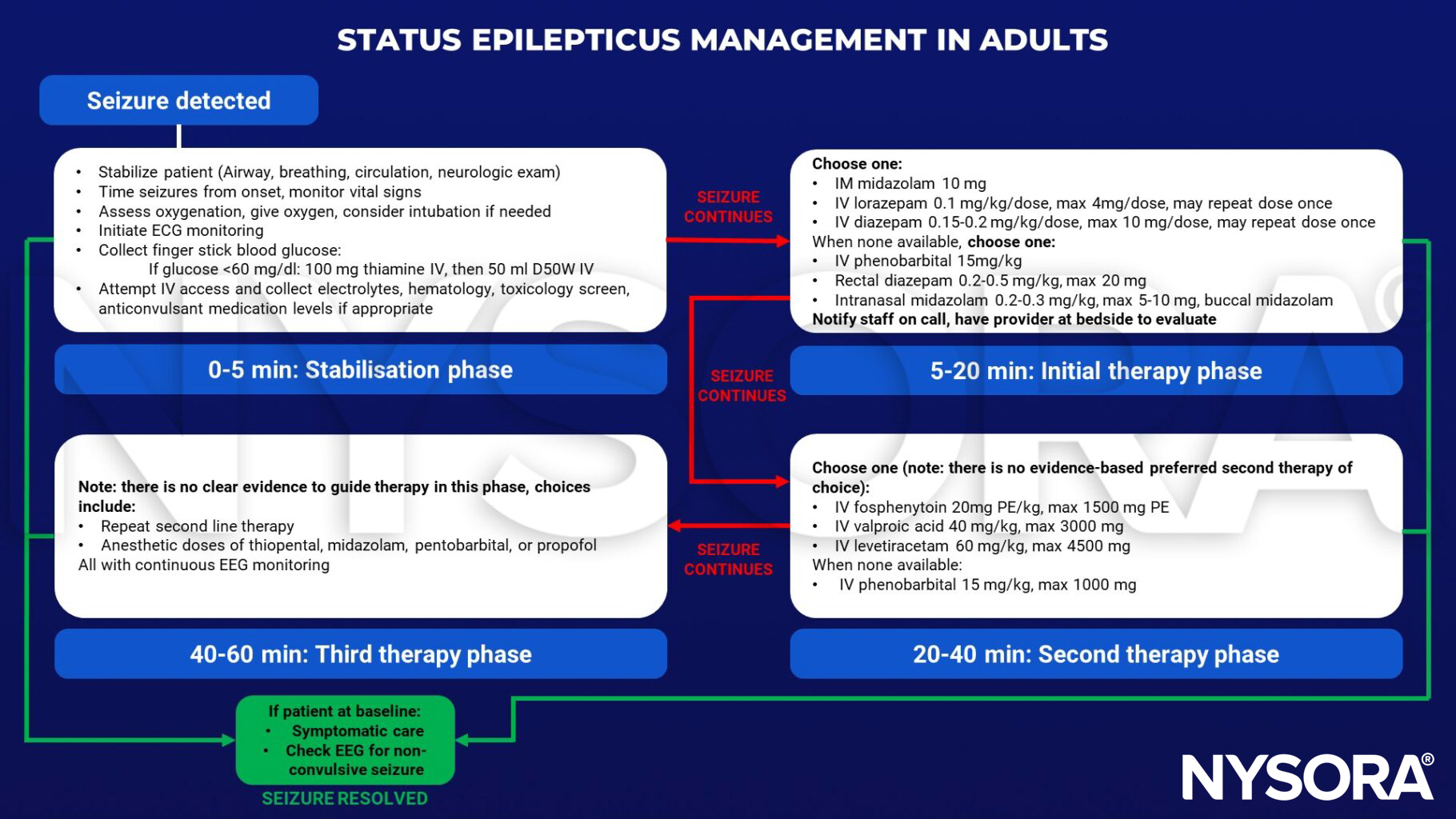
Status epilepticus medications: Overview
Rescue benzodiazepines
| Medication | Dose range (max dose) | Comments |
|---|---|---|
| IV lorazepam | 0.05-0.1 mg/kg/dose (2-4 mg) | May repeat dose once |
| Rectal diazepam | 0.2-0.5 mg/kg (20 mg) | Age 6 months - 5 years: 0.5 mg/kg Age 6-12 years: 0.3 mg/kg Age 12+ years: 0.2 mg/kg |
| Nasal midazolam | 0.2-0.3 mg/kg (5-10 mg) | <40 kg: 0.2-0.3 mg/kg >40 kg: give 10 mg (max dose), half the dose in each nostril |
| IM midazolam | 0.2-0.3 mg/kg (5-10 mg) | <13 kg: 0.2-0.3 mg/kg 13-40 kg: give 5 mg >40 kg: give 10 mg (max dose) |
| IV diazepam | 0.15-0.3 mg/kg (10mg) | Shorter duration compared to lorazepam Higher risk for respiratory depression |
Tier 2 medications
| Medication | Dose range (max dose) | Comments |
|---|---|---|
| Fosphenytoin | 20 mg PE/kg (1500 mg) | Drug levels quickly available for titration Avoid if known generalized epilepsy or Dravet syndrome Beware of hypotension and bradycardia Tissue extravasation is potentially dangerous |
| Levetiracetam | 60 mg/kg (4500 mg) | Also effective for myoclonic seizures |
| Valproic acid | 40 mg/kg (3000 mg) | Effective in juvenile myoclonic epilepsy, myoclonic status and absence status Caution in patients with liver dysfunction and select metabolic diseases (e.g., POLG1) |
| Phenobarbital | 10-20 mg/kg (1000 mg) | Drug of choice in newborns Beware of hypotension and respiratory depression May use in adults if previously used with status due to missed or held doses |
| Lacosamide | 5-10 mg/kg (400 mg) | Caution with cardiac issues, can prolong PR interval Use if previously used and status due to missed or held doses |
Suggested reading
- Glauser T, Shinnar S, Gloss D, et al. Evidence-Based Guideline: Treatment of Convulsive Status Epilepticus in Children and Adults: Report of the Guideline Committee of the American Epilepsy Society. Epilepsy Curr. 2016;16(1):48-61.
- Betjemann JP, Lowenstein DH. Status epilepticus in adults. Lancet Neurol. 2015;14(6):615-624.
- Perks A, Cheema S, Mohanraj R. Anaesthesia and epilepsy. BJA: British Journal of Anaesthesia. 2012;108(4):562-71.











