

Learning objectives
- Define and classify arrhythmias
- Describe the patient, anesthetic, and surgical risk factors for developing intraoperative arrhythmias
- Management of intraoperative arrhythmias
Definition and mechanisms
- Arrhythmias are accelerated, slowed, or irregular heartbeats caused by abnormalities in the electrical impulses of the myocardium
- 60% of patients may experience perioperative arrhythmias
- The majority are benign, but rhythm disturbance can be associated with potentially serious adverse outcomes
Classification
Bradyarrhythmia (HR <60 bpm)
- Sinus arrhythmia: Sinus bradycardia
- Conduction defects
- AV blocks
- First-degree AV block
- Second-degree AV block
- Third-degree AV block
- Intraventricular blocks
- Right bundle branch block
- Left bundle branch block
- Fascicular block
- Left anterior hemiblock
- Right anterior hemiblock
- Bifascicular block
- Trifascicular block
- AV blocks
Tachyarrhythmia (HR >100 bpm)
- Sinus arrhythmia: Sinus tachycardia
- Supraventricular arrhythmias
- Premature atrial contraction
- Supraventricular tachycardia
- Atrial flutter
- Atrial fibrillation
- Ventricular arrhythmias
- Premature ventricular contractions
- Ventricular tachycardia
- Ventricular fibrillation
- Torsade de pointes
Complications
- Blood clots (i.e., thromboembolism)
- Stroke
- Heart failure
- Sudden death
Risk factors
Patient factors
- Preexisting arrhythmias
- Coronary artery disease
- Hypertension
- Congestive heart failure
- Electrolyte disorders (especially potassium, magnesium, and calcium)
- Valvular heart disease
- Obstructive sleep apnea
- Medications:
- β2-agonists
- Theophylline
- Tricyclic antidepressants
- Less common causes:
- Thyroid disease (i.e., hypothyroidism, hyperthyroidism)
- Cardiomyopathies (including alcoholic)
- Myocarditis
- Trauma (myocardial or intracranial)
- Connective tissue disorders
- Smoking
- Drug and solvent abuse
Anesthetic factors
- Hypotension or hypertension (e.g., inadequate anesthesia)
- Hypoxia
- Hypercarbia
- Direct laryngoscopy and intubation
- Central nervous pressure lines (irritation by line tip; microshock hazard)
- Drugs
- Volatile anesthetic agents
- Local anesthetics
- Suxamethonium
- Pancuronium
- Multiple drugs prolong the QT interval (e.g., volatile agents, macrolide antibiotics, butyrophenone antipsychotics, amiodarone, and ondansetron)
- 4Hs 4Ts
- Hypovolemia, hypoxemia, hyper/hypokalemia (electrolyte disorders) and metabolic disorders (acidosis), and hypo/hyperthermia
- Tension pneumothorax, tamponade, toxins/drugs, thromboembolism (pulmonary/cardiac)
Surgical factors
- Catecholamines
- Endogenous (from any surgical stimulus)
- Exogenous (topical or infiltrated epinephrine)
- Autonomic stimulation
- Peritoneal and visceral traction
- Peritoneal insufflation
- Trigeminovagal reflexes (oculocardiac reflex)
- Laryngoscopy, bronchoscopy, esophagoscopy
- Carotid artery and thyroid surgery
- Direct stimulation of the heart during cardiac or thoracic surgery
- Embolism
- Thrombus
- Fat
- Bone cement
- Air
- Carbon dioxide
- Amniotic fluid
- Other
- Aortic cross-clamping
- Limb reperfusion
- Glycine intoxication
Treatment goals
- Prevent thromboembolism formation
- Control heart rate
- Correct the condition causing the arrhythmia
- Reduce other risk factors for heart disease and stroke
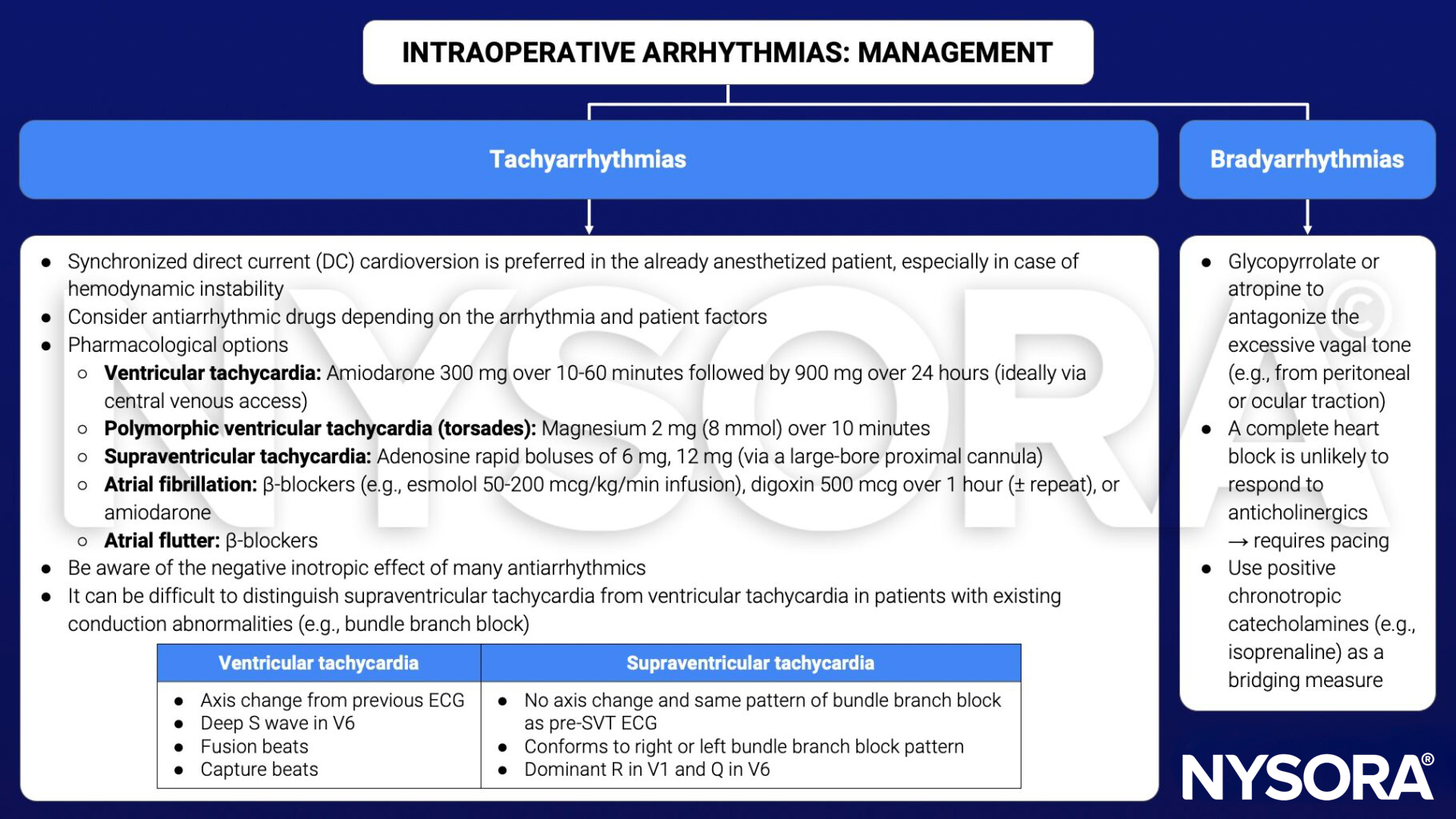
Management
- More than one factor is likely to contribute to the development of an intraoperative arrhythmia
- Identify the rhythm
- Evaluate its significance (in the context of)
- Coexisting medical problems and their treatment
- Surgical condition
- Operative procedure
- Anesthetic drugs and technique
- Hemodynamic effect of the arrhythmia and the risk of progression to a more serious arrhythmia
- Identify and correct any precipitating factors
- Take an ABC approach
- Treat the whole patient, not just the ECG
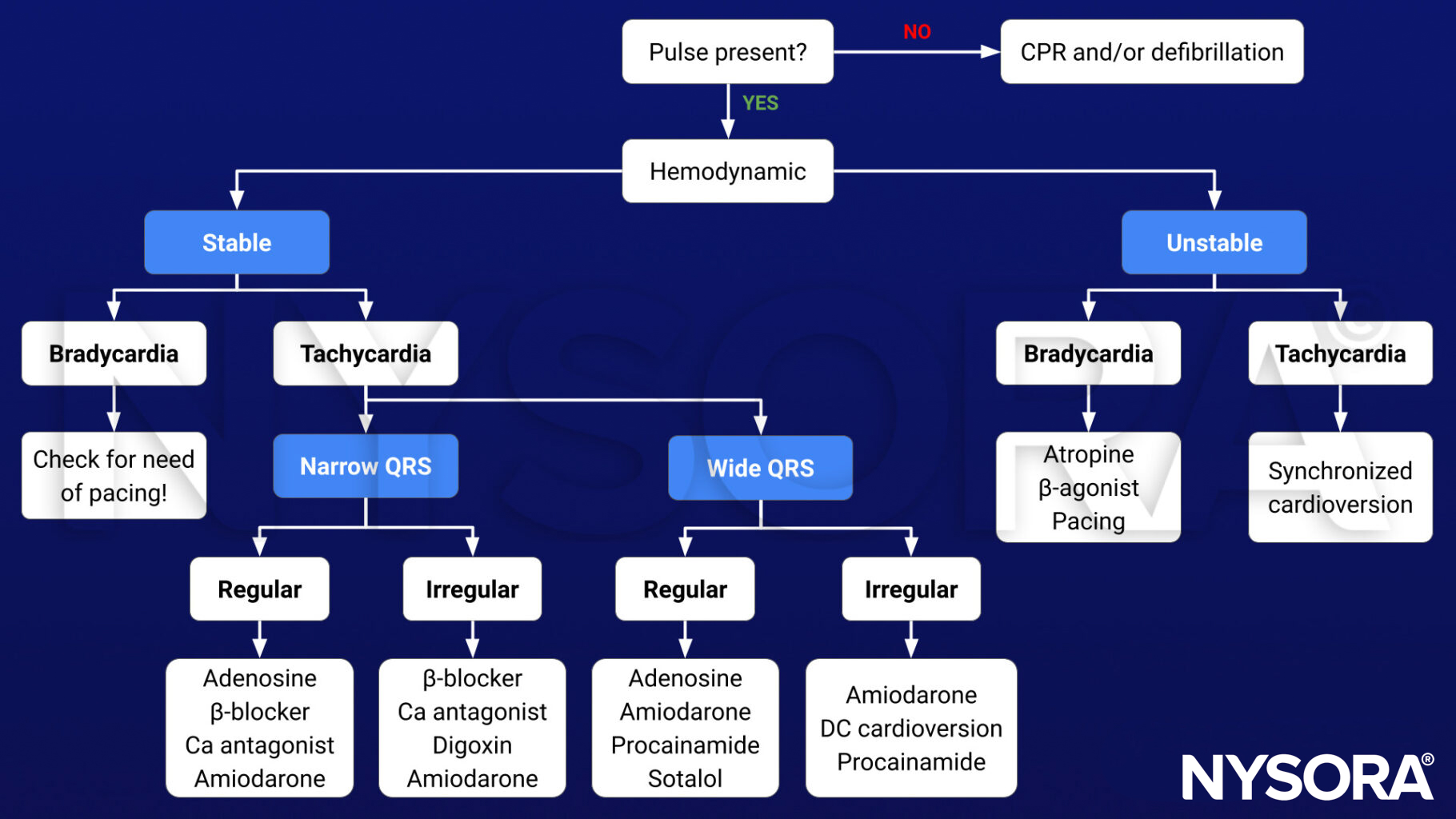
Algorithm
Prevention
- Keep surgical manipulations that can precipitate arrhythmias to a minimum
- An adequate depth of anesthesia may prevent or control intraoperative arrhythmias
- Prevent hypoxia, hypotension, hypovolemia, and hypothermia during surgery
Suggested reading
- Noor ZM. Md. Life-Threatening Cardiac Arrhythmias during Anesthesia and Surgery. Cardiac Arrhythmias – Translational Approach from Pathophysiology to Advanced Care. 2021. doi: 10.5772/intechopen.101371.
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 30 Management problems, Shelton C.
Clinical updates
Xie et al. (Anesthesiology, 2025) showed that intraoperative methadone, despite its long half-life and NMDA antagonism, does not increase clinically significant QT prolongation or perioperative arrhythmias compared with other opioids when used in appropriate doses and with standard monitoring. These data support methadone as a safe component of multimodal analgesia, provided electrolyte abnormalities are corrected, and concomitant QT-prolonging drugs are used cautiously.
- Read more about this study HERE.












