Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About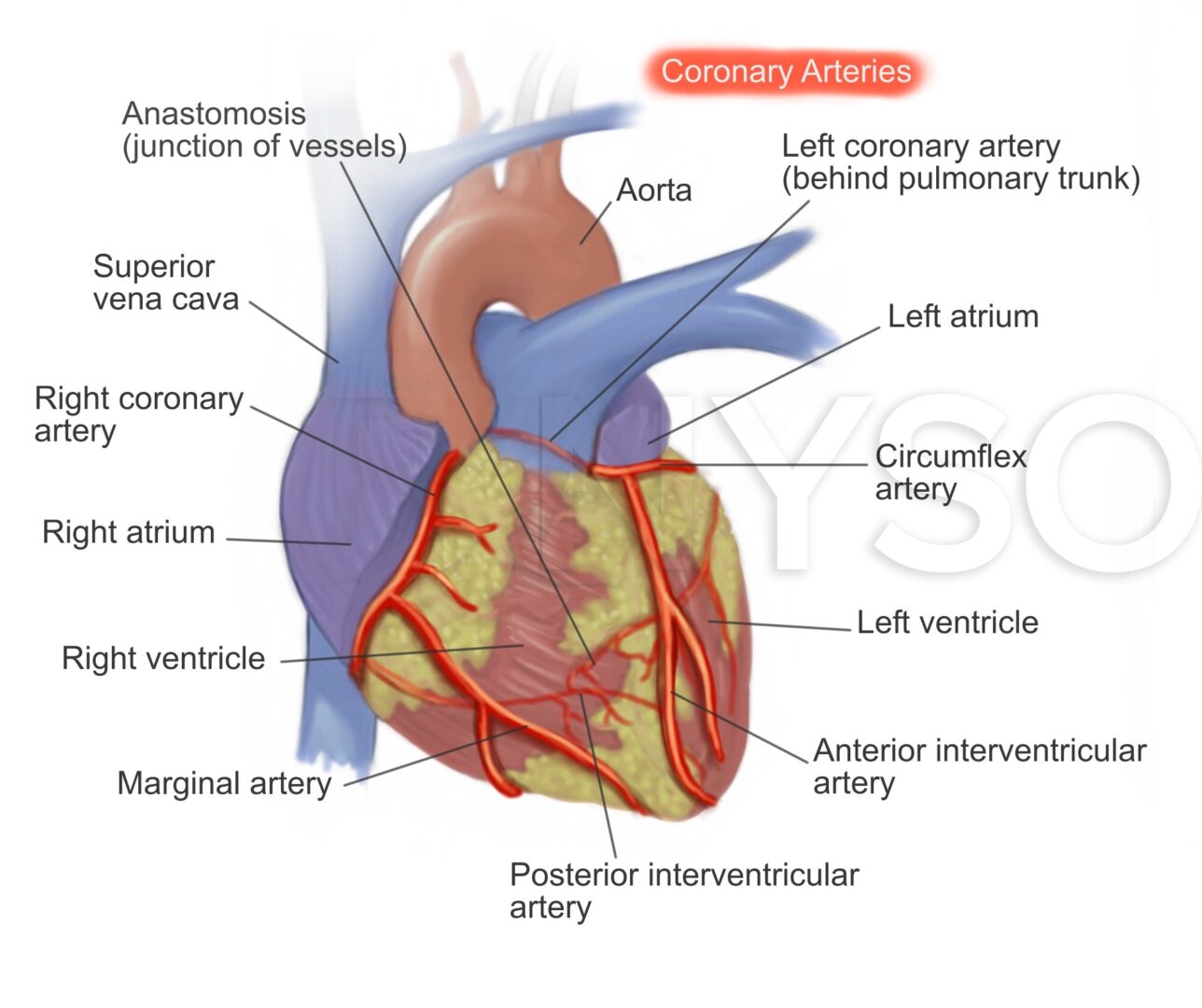
Learning objectives
- Describe the general pathology of coronary artery disease
- Describe the risk factors for coronary artery disease
- Manage patients with coronary artery disease
Definition & mechanisms
- Coronary artery disease or ischemic heart disease is characterized by obstruction of oxygen supply to the cardiac muscle
- Results in a range of complications, including myocardial infarction, dysrhythmias, heart failure, deteriorating ventricular function, and sudden death
- May also coexist with other cardiac pathologies, including valvular lesions and cardiomyopathies
- Atheromatous disease remains the most common cause
- Ischemia results when myocardial oxygen demand increases beyond supply or when there is a rupture of a plaque which can precipitate thrombosis and result in complete occlusion of an artery
Risk factors
| Unmodifiable | Advancing age |
| Male gender | |
| Family history of premature coronary artery disease | |
| Premature menopause | |
| Ethnicity (e.g. higher in those from the Indian subcontinent) | |
| Modifiable | Smoking |
| Diabetes mellitus | |
| Hypertension | |
| Obesity | |
| Sedentary lifestyle |
|
| High cholesterol (specifically a high ratio of low- to high-density lipoprotein) |
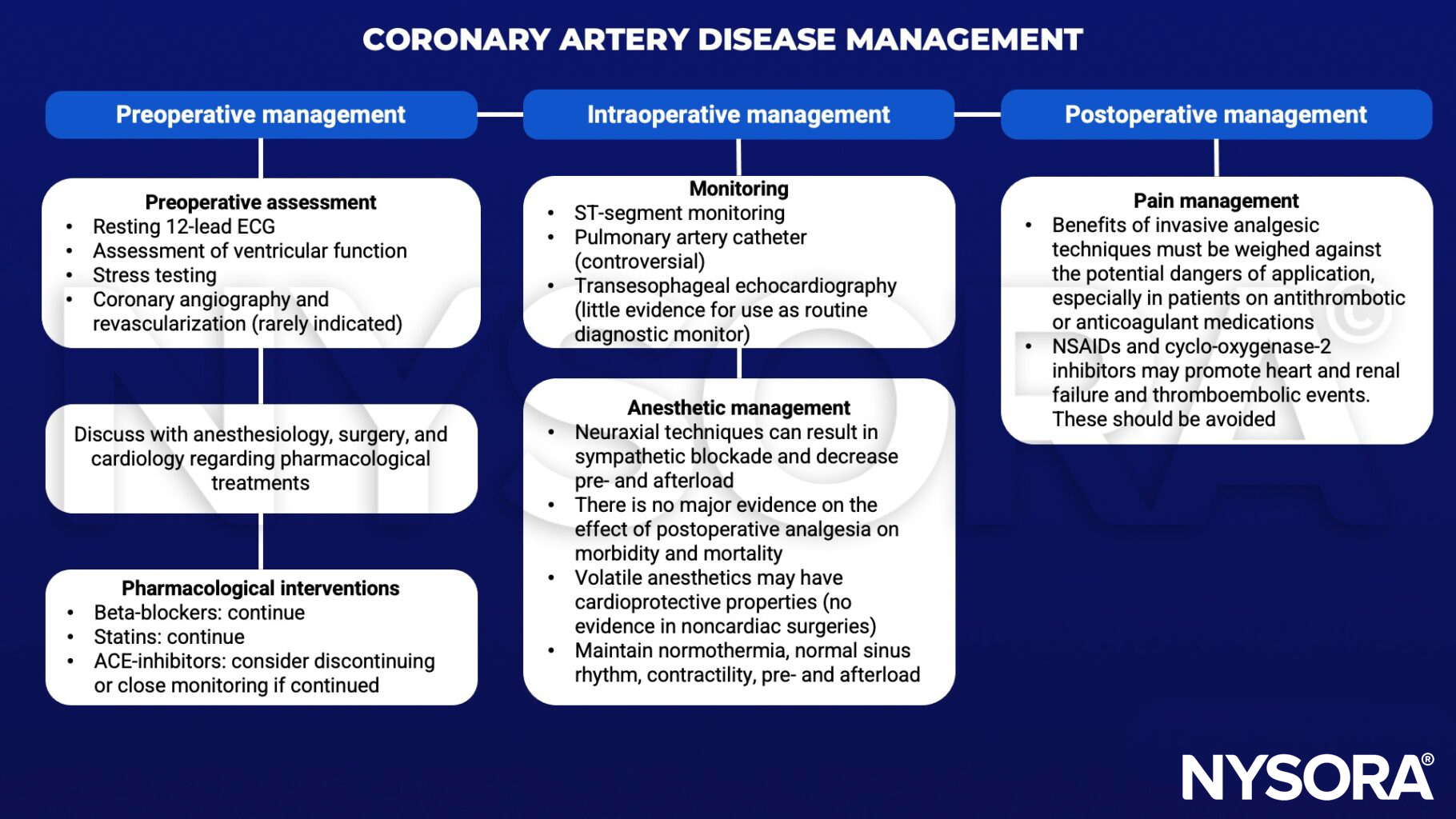
Management
Suggested reading
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
Clinical updates
Camaj et al. (JAMA Cardiology, 2025) provide a comprehensive review of drug-coated balloon (DCB) angioplasty as an alternative to drug-eluting stents (DES) in coronary artery disease, emphasizing that DCBs deliver homogeneous antiproliferative therapy without permanent metal implantation, thereby preserving vessel anatomy and vasomotion and enabling positive remodeling. They highlight established efficacy in in-stent restenosis (the only current FDA-approved coronary indication in the US), expanding evidence in small-vessel disease and selected de novo lesions, emerging roles in long lesions and bifurcations, and the importance of meticulous lesion preparation and short-course DAPT (≈approximately 1 month) to optimize outcomes.
Kittleson (Annals of Internal Medicine, 2025) provides an updated, guideline-aligned framework for chronic coronary artery disease (CCAD), emphasizing risk-stratified diagnosis using pretest probability and coronary artery calcium scoring (Agatston ≥100 suggesting ≥15% likelihood of obstructive CAD) and favoring stress imaging over exercise ECG in intermediate–high risk patients, with CCTA preferred in those <65 years. The review details contemporary guideline-directed medical therapy, including LDL-C targets <70 mg/dL (or <55 mg/dL if very high risk) with early addition of ezetimibe or PCSK9 inhibitors, incorporation of SGLT2 inhibitors and GLP-1 receptor agonists for patients with diabetes (and semaglutide benefit even without diabetes in SELECT), BP goals <130/80 mm Hg, and selective use of colchicine in very high-risk patients, while reinforcing that routine revascularization does not reduce MI or mortality compared with optimal medical therapy but is appropriate for lifestyle-limiting angina despite GDMT.
Holmes et al. (Journal of Cardiovascular Development and Disease, 2025) provide a comprehensive review of anesthetic management for minimally invasive coronary artery bypass grafting (MI-CABG), emphasizing the need for tailored perioperative strategies to manage one-lung ventilation, heart-positioning–related hemodynamic instability, and limited surgical exposure, without routine cardiopulmonary bypass. They highlight the importance of careful patient selection (including assessment of LV function, pulmonary reserve, and vascular access), proactive hemodynamic support during distal anastomoses, and multimodal, often regional, analgesia to facilitate early extubation and mobilization, underscoring the anesthesiologist’s central role in optimizing outcomes as MI-CABG adoption expands.
Chen et al. (Nature Medicine, 2025) developed a meta-prediction framework integrating ~2,000 demographic, clinical, biometric, and genetic features, including multiple polygenic risk scores, into a 10-year incident CAD model that achieved an AUROC of 0.84 in the UK Biobank and 0.81 in external validation with All of Us, outperforming standard clinical scores. The model identified genetically defined risk subgroups with differential responses to LDL, HbA1c, and SBP lowering, demonstrating that individuals with higher polygenic risk derive substantially greater absolute risk reduction from aggressive lipid and risk-factor control, enabling personalized prevention strategies.