
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the physiology, causes, and effects of metabolic acidosis
- Diagnose metabolic acidosis
- Manage metabolic acidosis
Background
- Metabolic acidosis is a disturbance in the homeostasis of plasma acidity
- Any process that increases the serum hydrogen ion concentration is a distinct acidosis
- A patient can have multiple acidoses contributing to the decrease of serum pH
- Adicosis can be either respiratory (changes in CO2) or metabolic (changes in bicarbonate)
- Metabolic acidosis is characterized by an increase in serum hydrogen ion concentration resulting in serum bicarbonate (HCO3) <24 mEq/L
- May be associated with organ failure, especially respiratory and cardiovascular
- Can be acute or chronic
Etiology
- Classification of metabolic acidosis is based on the presence or absence of an anion gap (concentration of unmeasured serum anions)
- Sodium, the main plasma cation, is balanced by the sum of the anions bicarbonate and chloride in addition to the unmeasured anions (e.g., lactate, acetoacetate), which represent the anion gap
- Anion gap metabolic acidosis is often caused by anaerobic metabolism and lactic acid accumulation
- Non-gap metabolic acidosis is primarily caused by the loss of bicarbonate (e.g., diarrhea, renal tubular acidosis)
- Causes:
| Anion gap metabolic acidosis | Non-gap metabolic acidosis associated with normal or high serum K+ | Non-gap metabolic acidosis associated with low serum K+ |
|---|---|---|
| Acute kidney injury | Administration of HCl or precursors | Diarrhea |
| Chronic kidney disease | Administration of cationic amino acids | intestinal, pancreatic, or biliary fistula |
| Diabetic ketoacidosis | Chronic kidney disease | Proximal renal tubular acidosis |
| Alcoholic ketoacidosis | Adrenal insufficiency (primary or secondary) | Distal renal tubular acidosis |
| Lactic acidosis | Hyporeninemic hypoaldosteronism | Ureterosigmoidostomy |
| Salicylate intoxication | Hyperkalemic distal renal tubular acidosis | Ureteroileostomy |
| Toxic alcohol intoxication (methanol, ethylene glycol, diethylene glycol, propylene glycol) | Pseudoaldosteronism type I | Diabetic ketoacidosis |
| Pyroglutamic acidosis | Pseudoaldosteronism type II (Gordon’s syndrome) | Toluene intoxication |
| Fasting ketoacidosis | Drugs (spironolactone, prostaglandin inhibitors, triamterene, amiloride, trimethoprim, pentamidine, ciclosporin) | Lactic acidosis |
| Toluene intoxication |
Adverse effects
| Acute metabolic acidosis | Chronic metabolic acidosis |
|---|---|
| Impaired leukocyte function | Generation or exacerbation of bone disease |
| Predisposition to ventricular arrhythmias | Growth retardation (in children) |
| Arterial vasodilation and hypotension | Impaired glucose tolerance |
| Resistance to action of infused catecholamines | Acceleration of progression of kidney disease |
| Resistance to action of insulin | Increased muscle wasting |
| Suppression of lymphocyte function | Reduced albumin synthesis |
| Impaired cellular energy production | Enhanced production of β2-microglobulin |
| Stimulation of apoptosis | |
| Changes in mental status | |
| Stimulation of interleukin production | |
| Alteration in oxygen binding to hemoglobin | |
| Venoconstriction | |
| Decreased cardiac contractility and cardiac output |
Diagnosis
- History: Identify potential causes (vomiting, diarrhea, medications, possible overdoses, chronic conditions such as diabetes mellitus)
- Physical examination: dry mucus membranes in diabetic ketoacidosis, compensatory hyperventilation
- Lab tests;
- Blood pH <7.35
- pCO2:
- >40-45: respiratory acidosis
- <40: metabolic acidosis
- Anion gap
- Anion gap = Na+ – (Cl- + HCO3-)
- Normal anion gap = 12
- Anion gap >12: Anion gap metabolic acidosis
- Respiratory compensation
- Winter’s formula: Expected CO2 = (HCO3- x 1.5) + 8 +/- 2
- If pCO2 is within the predicted range, there is no additional respiratory disturbance
- If pCO2 is greater than expected, there is an additional respiratory acidosis
- If pCO2 is less than expected, there is an additional respiratory alkalosis
- Additional metabolic disturbances
- If anion gap is present, determine delta gap
- Delta gap = Delta anion gap – Delta HCO3- = (anion gap – 12) – (24 – HCO3-)
- Delta gap < -6: Non anion gap metabolic acidosis
- Delta gap >6: underlying metabolic alkalosis
- Delta gap between -6 and 6: only anion gap metabolic acidosis
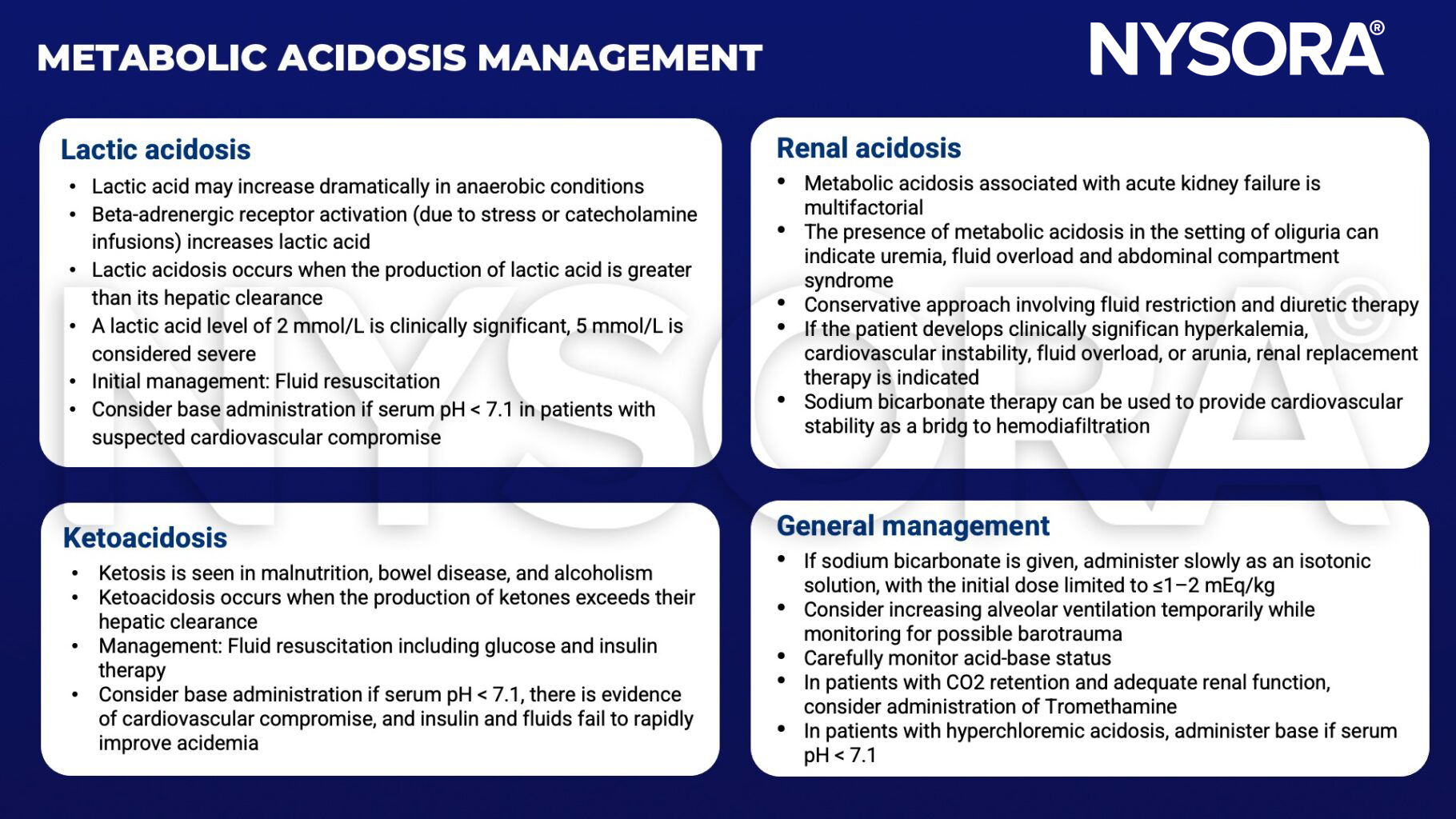
Management
- Address the cause of acidosis
- Fluid resuscitation and electrolyte imbalance correction for sepsis and diabetic ketoacidosis
- Antidotes for poisoning, dialysis, antibiotics, bicarbonate administration
Suggested reading
- Burger MK, Schaller DJ. Metabolic Acidosis. [Updated 2022 Jul 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482146/
- Fleisher, Lee A., and Stanley H. Rosenbaum. Complications in Anesthesia. Elsevier, 2018.
- Kraut, J., Madias, N. Metabolic acidosis: pathophysiology, diagnosis and management. Nat Rev Nephrol 6, 274–285 (2010).
Clinical updates
Brekke et al. (2025, EJA) report that patients with type 2 diabetes receiving SGLT2 inhibitors undergoing cardiac surgery have a significantly higher risk of postoperative metabolic acidosis, characterized by lower base excess and higher (often modest) anion gaps without elevated lactate, consistent with ketosis. Notably, 41% of SGLT2-i–treated patients without renal failure developed clinically relevant acidosis within 12 hours postoperatively, and SGLT2-i use was an independent predictor of acidosis despite drug cessation before surgery. These findings emphasize that metabolic acidosis may be masked by normoglycemia and normal lactate, underscoring the need for perioperative monitoring of base excess, anion gap, and ketones, and early treatment with insulin, dextrose, and volume optimization in at-risk patients.












