Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About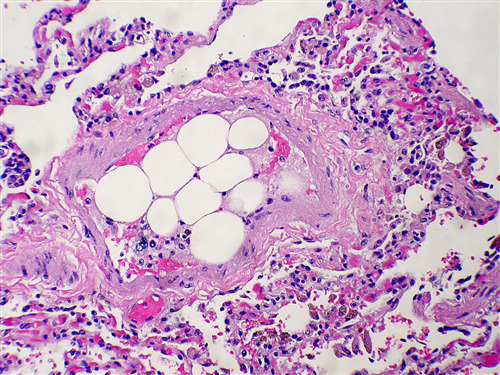
Learning objectives
- Recognize fat embolism syndrome (FES)
- Describe the presenting clinical features in patients with suspected FES
- Explain the management of FES, including the limited drug treatments
Definition and mechanism
- The presence of fat globules within the lung parenchyma or peripheral microcirculation
- Causes direct tissue damage as well as the induction of a systemic inflammatory response
- Result in pulmonary, cutaneous, neurological, and retinal symptoms
- Estimated to occur in 1-10% of patients
- Mortality is 10-20%
Signs and symptoms
| Respiratory | Tachypnea Hypoxemia Acute Respiratory Distress Syndrome |
| Neurological | Confusion Seizures Altered level of consciousness Focal neurological deficits |
| Dermatological | Petechial rash |
| Systemic | Fever |
| Cardiovascular | Tachycardia Hypotension Intraoperative arrhythmias Myocardial ischemia Pulmonary hypertension (PH) Right-sided heart failure |
| Ophthalmic | Purtscher’s retinopathy (cotton wool exudates, macular edema and hemorrhage) |
| Renal | Oliguria Proteinuria Lipiduria Hematuria |
| Hepatic | Jaundice |
| Haematological | Perioperative anemia Thrombocytopenia Coagulopathy Fat macroglobulinemia |
Causes
- Trauma to long bone/pelvis
- Prosthetic joint replacement
- Liposuction
- Bone marrow harvest or transplant
- Bone tumor lysis
- Acute pancreatitis
- Hepatic necrosis and fatty lever
- Acute sickle cell crisis
- Major soft tissue injury
- Recent orthopedic procedure
- Recent lipid infusion
- Severe burns
Diagnosis
One major and 4 minor of Gurd’s Diagnostic Criteria are proposed, together with fat macroglobulinemia, as sufficient to diagnose fat embolism syndrome
Gurd’s diagnostic criteria
| Diagnosis | Criteria |
|---|---|
| Major criteria | Respiratory insufficiency Cerebral involvement Petechial rash |
| Minor criteria | Tachycardia Fever Jaundice Retinal changes Renal changes ↓ Hemoglobin Thrombocytopenia ↑ Erythrocyte sedimentation rate Fat globulus in sputum |
| Laboratory findings | ↓ in hematocrit at 24 to 48 hours Thrombocytopenia Fat globulus in blood and urine Fat macroglobulinemia raised free fatty acids and triglyceride in serum |
Management
- Respiratory support: intubation/ventilation, indications for respiratory support:
- Sustained SaO2 <90% and PaO2 <8 kPa on oxygen
- Respiratory rate of >35 breaths/min
- Hemodynamic support:
- Maintain a systolic blood pressure > 90 mmHg
- Avoid hypovolemia with fluid resuscitation and vasopressors
- Apply invasive monitoring
- TEE
- Early surgical stabilization of fractures
- Perform operative correction rather than traction alone
- Limit the intraosseous pressure during an orthopedic procedure
Pharmacological treatment
- Corticosteroids may reduce the risk of a fat embolism in patients with long bone fractures of the lower limbs
- Heparin clears lipemic serum by stimulating lipase activity, thereby reducing pulmonary complications
- Albumin use is considered potentially therapeutic in its ability to bind free fatty acids
Suggested reading
- Luff D, Hewson DW. Fat embolism syndrome. BJA Educ. 2021;21(9):322-328.
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.