
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About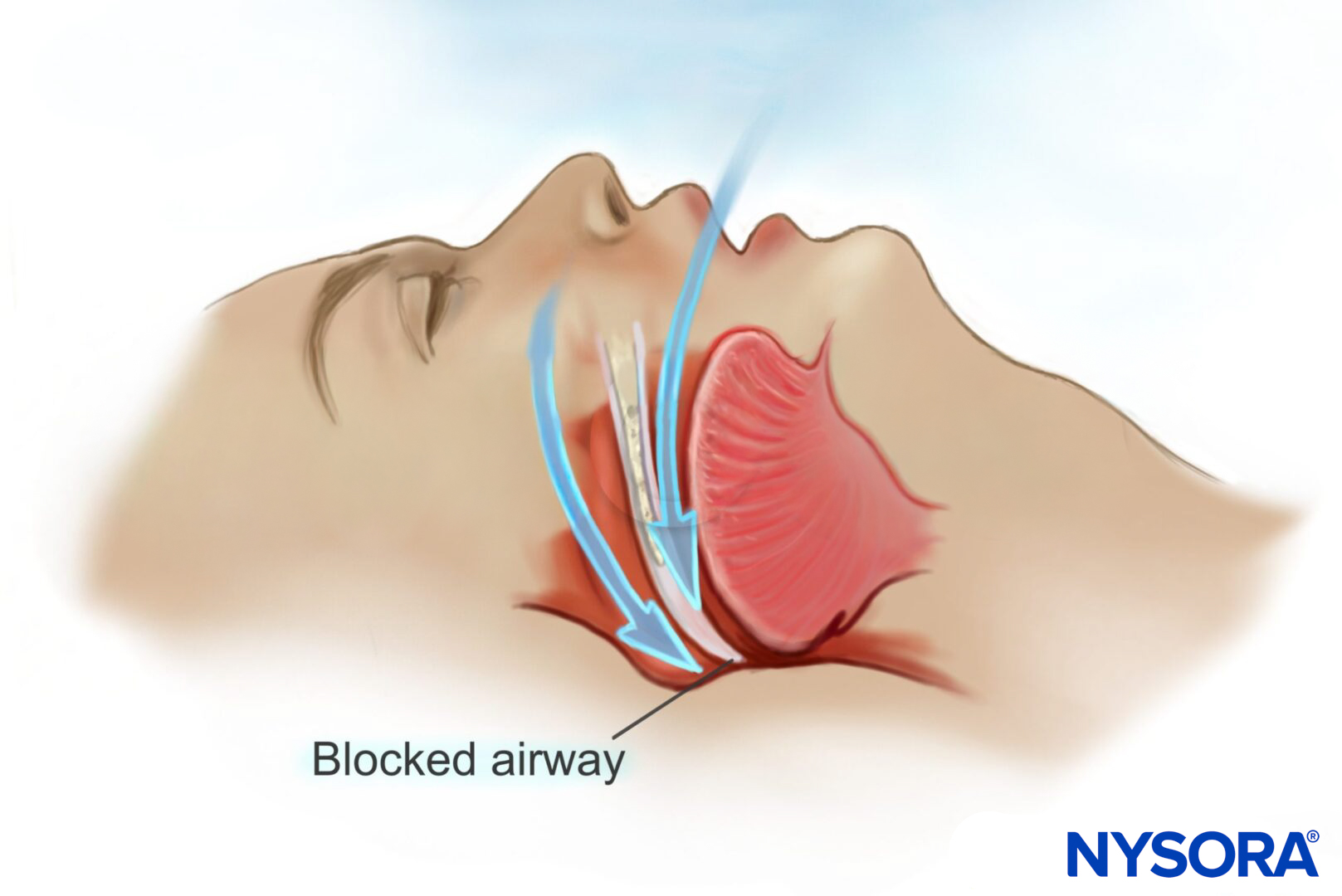
Learning objectives
- Manage a patient with obstructive sleep apnea (OSA) in the perioperative period
Definition and mechanisms
- Obstructive sleep apnea (OSA) is a disorder in which a person frequently stops breathing during their sleep due to obstruction of the upper airway
- This obstruction is caused by an inadequate motor tone of the tongue and/or airway dilator muscles and is exaggerated by excessive adipose tissue
- OSA accompanied by excessive daytime sleepiness is termed OSA syndrome (OSAS)

Background
- OSA affects 5-10% of the general population but is twice as prevalent in the population undergoing surgery
Predisposing factors
- Obesity
- Age 40-70
- Male gender
- Alcohol abuse
- Smoking
- Pregnancy
- Low physical activity
- Unemployment
- Neck circumference > 40 cm
- Tonsillar and adenoidal hypertrophy
- Craniofacial abnormalities (e.g., Pierre Robin, Down’s syndrome)
- Neuromuscular disease
Medical consequences
OSA is associated with
Neurocognitive
- Increased risk of cerebrovascular accidents with poorer outcomes
- Psychosocial problems
- Decreased cognitive function
- Depression
Endocrine
- Impaired glucose tolerance
- Dyslipidemia
- Increased adrenocorticotropic hormone and cortisol concentrations
- Testicular and ovarian dysfunction
Cardiovascular
- Hypertension
- Brady- and tachyarrhythmias
- Pulmonary hypertension
- Congestive heart failure
- Myocardial infarction
Treatment
- Weight loss is the preferred treatment for obese patients with OSA
- Continuous positive airway pressure (CPAP) therapy may reduce the risk of cardiac and cerebrovascular events, this effect is most pronounced in non-obese patients
- Surgical uvulo-palato-pharyngoplasty and various supportive airway devices promoting mandibular advancement can be offered to selected patients but have lower efficacy than weight loss and CPAP
Anesthesiologic implications
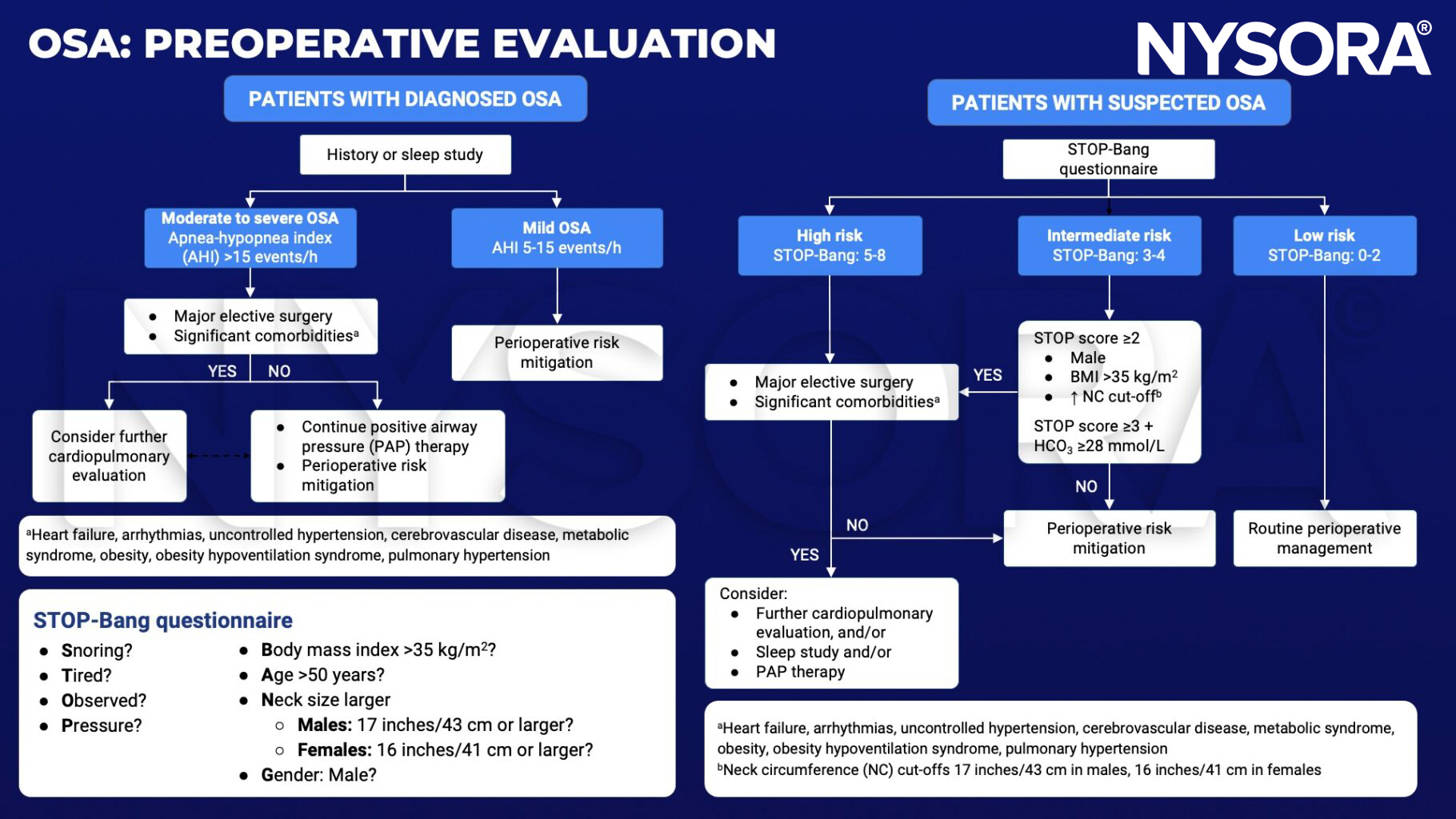
- Assess the patient preoperatively for conditions associated with OSA
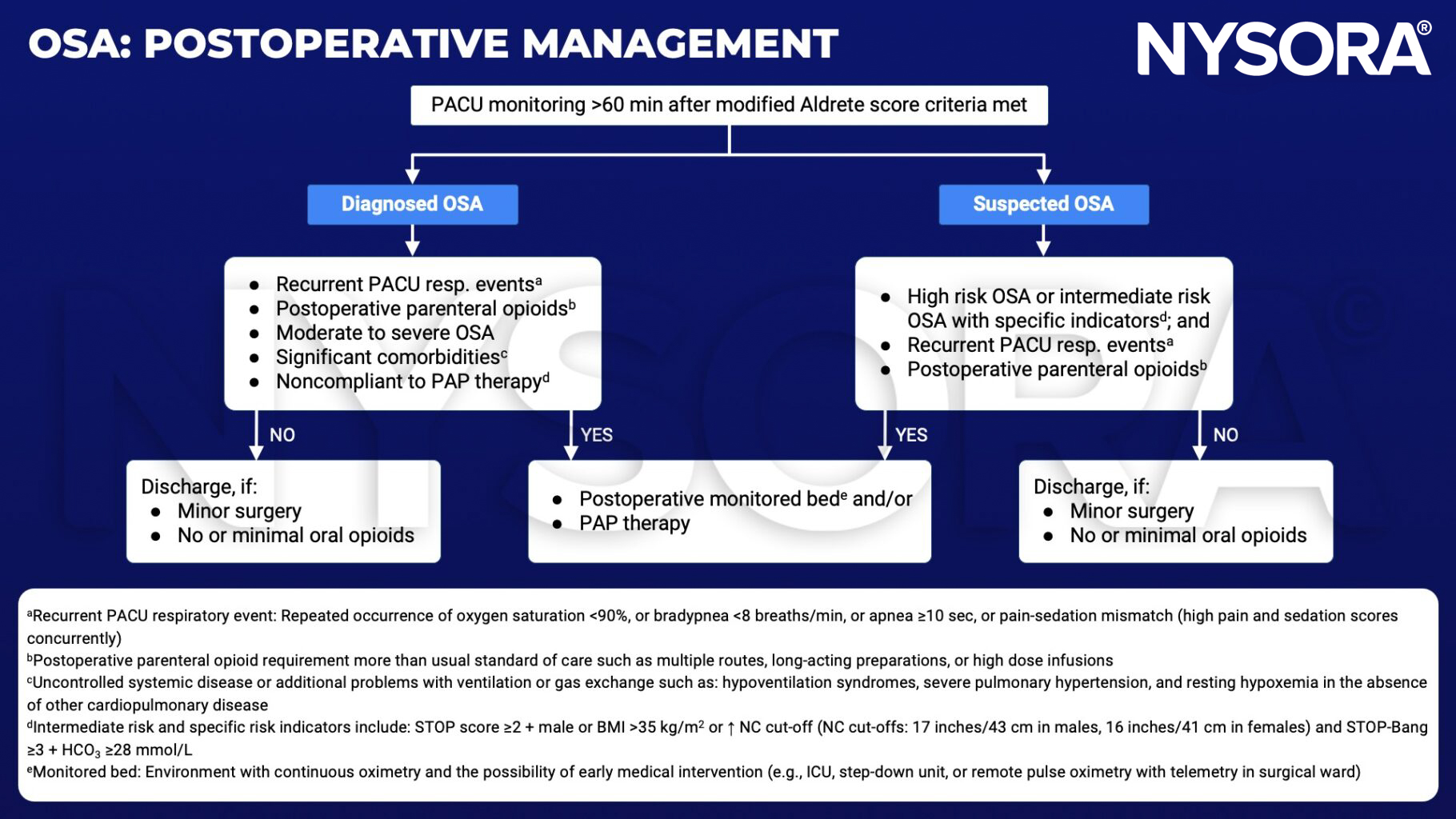
- Continue CPAP treatment during hospital admission and in the recovery room
- Avoid the administration of sedative medication unless the patient is properly monitored
- OSA is associated with difficult intubation so plan accordingly
- Use locoregional techniques where possible
Suggested reading
- Martinez G, Faber P. Obstructive sleep apnoea. Continuing Education in Anaesthesia Critical Care & Pain. 2011;11(1):5-8.
Clinical updates
Kristensen et al. (Current Opinion in Anesthesiology, 2025) emphasize that patients with obstructive sleep apnea (OSA) undergoing head and neck surgery have an increased risk of difficult mask ventilation, rapid desaturation, and failed intubation, necessitating structured airway planning and early use of advanced techniques. The authors highlight ramped positioning, apneic oxygenation, and first-line use of video laryngoscopy, with awake tracheal intubation recommended when airway obstruction risk is high or ventilation is uncertain. They further emphasize postoperative vigilance, as airway edema and residual obstruction increase the risk of reintubation, and suggest delayed extubation for high-risk patients who are ready for immediate airway rescue.
- Read more about this study HERE.
Ajetunmobi et al. (Anesthesia & Analgesia, 2025) found that in 120 morbidly obese adults with OSA undergoing bariatric surgery, sugammadex (2 mg/kg) did not shorten recovery compared with neostigmine 2.5 mg + glycopyrrolate, with similar median time to OR discharge and no meaningful differences in extubation time or other early recovery milestones. PACU desaturation events were uncommon and similar, and there were no severe pulmonary complications, while sugammadex was far more expensive, supporting neostigmine as a clinically equivalent, cost-effective default in routine cases.
- Read more about this study HERE.










