Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the overall mechanisms of cardiac tamponade
- Recognize sings and symptoms of cardiac tamponade
- Diagnose cardiac tamponade
- Anesthetic management of patients with cardiac tamponade
Definition & mechanisms
- Cardiac tamponade is characterized by compression of the heart chambers caused by an accumulation of fluid in the pericardial space
- Common causes:
- Pericarditis
- Tuberculosis
- Trauma
- Malignancy
- Iatrogenic, e.g., after cardiac surgery and invasive procedures
- Intrapericardial pressure increases, causing an increase in right (RV) and left ventricular (LV) filling pressures
- Increased intrapericardial pressure eventually compresses all the cardiac chambers causing a decrease in cardiac output
- Tamponade leads to an exaggerated shift of the interventricular septum to the left during inspiration resulting in impairment of LV filling
- Decrease in systemic arterial pressure of >10 mmHg during inspiration (pulsus paradoxus)
- Crucial factors in the development of tamponade:
- Rate of fluid accumulation relative to pericardial stretch
- Presence or absence of compensatory mechanisms
- Gradually developing effusions are largely asymptomatic, rapidly accumulating effusions can present with tamponade
Signs & symptoms
- Symptoms:
- Dyspnea (usually the first and most sensitive)
- Orthopnea
- Chest discomfort
- Clinical manifestations are consistent with low cardiac output and high central venous pressure:
- Low mean arterial pressure
- Cool peripheries
- Signs of poor end-organ perfusion (e.g., low urine output)
- Palpating the pulse reveals an apparent variation in pulse volume due to pulsus paradoxus
- Jugular venous pressure is typically increased, with distended neck veins apparent
- Sympathetic tone is increased and manifests as tachycardia, diaphoresis, anxiety and poor distal perfusion
- A pericardial rub might be heard on auscultation in patients with inflammatory pericardial disease
Diagnosis
- Chest X-ray: Enlarged globular cardiac silhouette in chronic large pericardial effusions
- ECG:
- QRS complexes may be lower
- Sinus tachycardia is common
- Atrial dysrhythmias may be present
- Beat-to-beat variation in both amplitude and axis of the QRS complexes may be present in patients with large effusions
- Transthoracic (TTE) or transesophageal echocardiography (TEE): determine the size, location, and hemodynamic effects of the pericardial effusion:
- Effusions up to 10 mm in thickness during diastole are considered small, between 10 and 20 mm moderate, and greater than 20 mm large
- Collapse of the cardiac chambers
- Inferior vena cava dilatation
- Increased respiratory variation in the intracardiac blood flow measured with Doppler
- Excessive leftward shift of the interventricular septum during spontaneous inspiration
- Differential diagnoses:
- Epicardial fat
- Pleural effusions
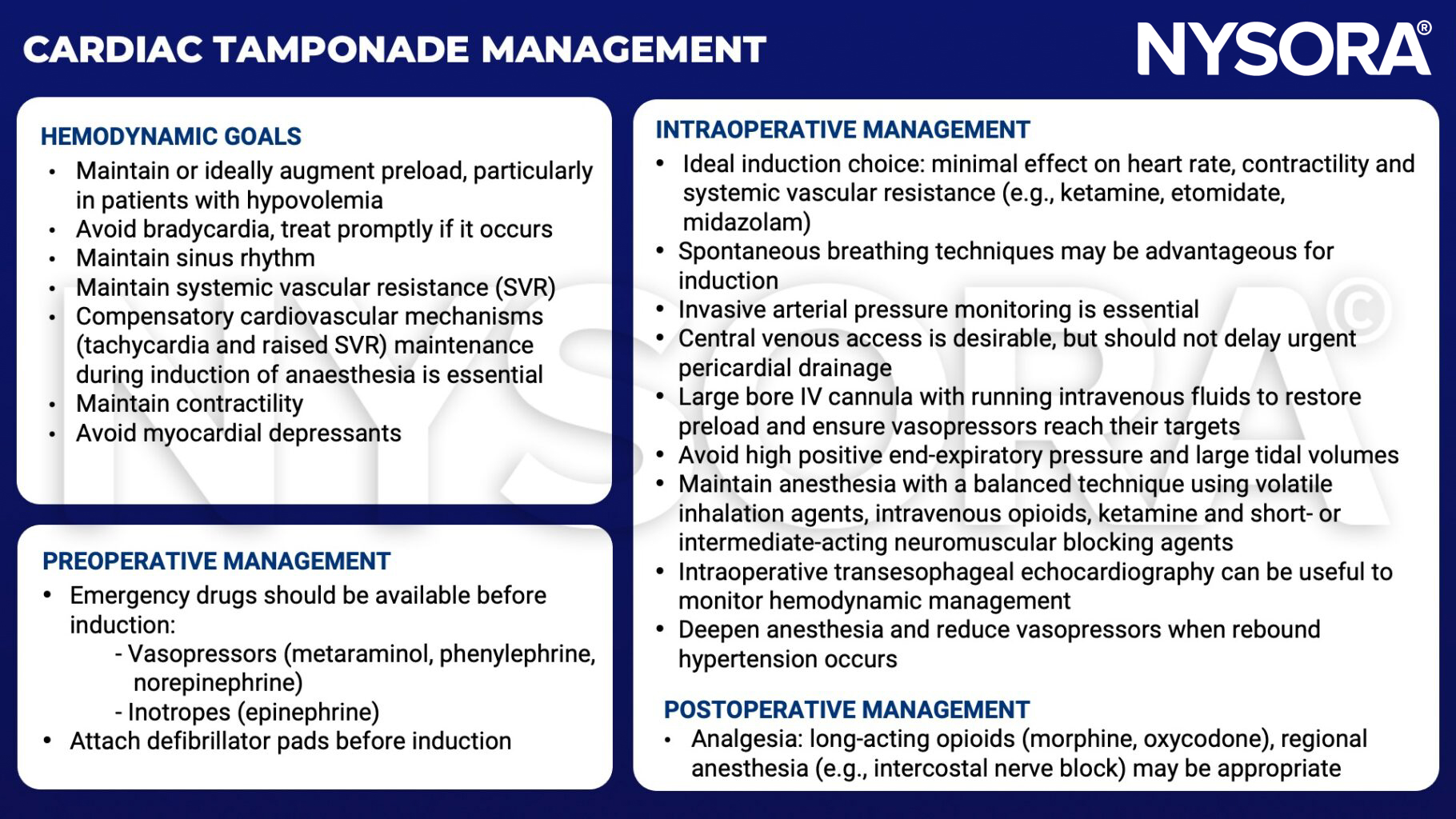
Management
Keep in mind
- Cardiac tamponade is an emergency requiring relief of the pressure effect of the pericardial fluid
- This is achieved by drainage procedures, which can be percutaneous or open surgical techniques
Suggested reading
- Madhivathanan PR, Corredor C, Smith A. Perioperative implications of pericardial effusions and cardiac tamponade. BJA Educ. 2020;20(7):226-234.
- Clinical Anesthesiology: 5th Edition, Morgan, GE, Mikhail, MS, Murray, MJ. Anesthesia for Cardiac Surgery: Cardiac Tamponade. 474-76.
- Essence of Anesthesia Practice: 4th Edition, Fleisher, LA, Roizen, Michael, F, Roizen. Cardiac Tamponade. 76.
Clinical updates
- Royster et al. (Anesthesiology, 2026) provide a detailed physiologic framework for cardiac tamponade, emphasizing its respirophasic nature and the three progressive hemodynamic phases as pericardial pressure equilibrates with right- and then left-sided diastolic pressures, with pulsus paradoxus becoming more prevalent in advanced stages. They highlight important updates for anesthesiologists, including recognition and management of low-pressure tamponade, the nuanced role of positive-pressure ventilation, and the risk of pericardial decompression syndrome after rapid drainage.
- Reference: Royster RL et al. Cardiac Tamponade: Impact of Pathophysiology on Clinical Practice. Anesthesiology. 2026;144:461-472.