Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe common causes of VAE and high-risk procedures
- Prevent VAE
- Manage VAE
Definition and mechanisms
- Venous air embolism (VAE) is caused by the ingress of gas into the venous system, most commonly air
- Rare iatrogenic complication in a wide range of clinical scenarios involving line placement, trauma, barotrauma, and several types of surgical procedures including cardiac, vascular, and neurosurgery
- Traditionally, surgery and trauma were the most significant causes of air embolism; now, endoscopy, angiography, tissue biopsy, thoracocentesis, hemodialysis, and central/peripheral venous access comprise a greater proportion
- May cause end-organ ischemia or infarction.
- May cause direct endothelial injury leading to the release of inflammatory mediators, activation of the complement cascade, and in situ thrombus formation
Signs & symptoms
- The presentation of VAE is dependent on the rate and volume of air entrained; Signs include:
- Apnea
- Hypoxia
- Cardiopulmonary collapse
- Tachypnea
- Tachycardia
- Hypotension
- Altered mental status
- Decreased conscious level
- Focal neurological deficits
- ‘Mill wheel’ murmur on cardiac auscultation
- Pulmonary edema may develop later
- Light-headedness, vertigo
- Breathing difficulties
- Shortness of breath
- Chest pain
- Sense of impending death
- ETCO2 falls
- Arterial oxygen saturation falls
- Hypoxemia
- ECG abnormalities (tachyarrhythmias, atrioventricular block, signs of right ventricular strain, ST-segment elevation or depression, non-specific T wave changes)
- Transesophageal echocardiography is the most reliable monitor to detect VAE
Prevention
- Patient positioning: avoid the sitting position and Trendelenburg position during the insertion of central venous catheters, try to prevent a negative gradient between the open site veins and the right atrium (increasing right atrial pressure via leg elevation and using the “flex” option on the operating table control)
- Holding ventilation when placing tunnel catheters
- Removal of temporary catheter synchronized with active exhalation/Valsalva maneuver or positive end-expiratory pressure
- Avoid nitrous oxide
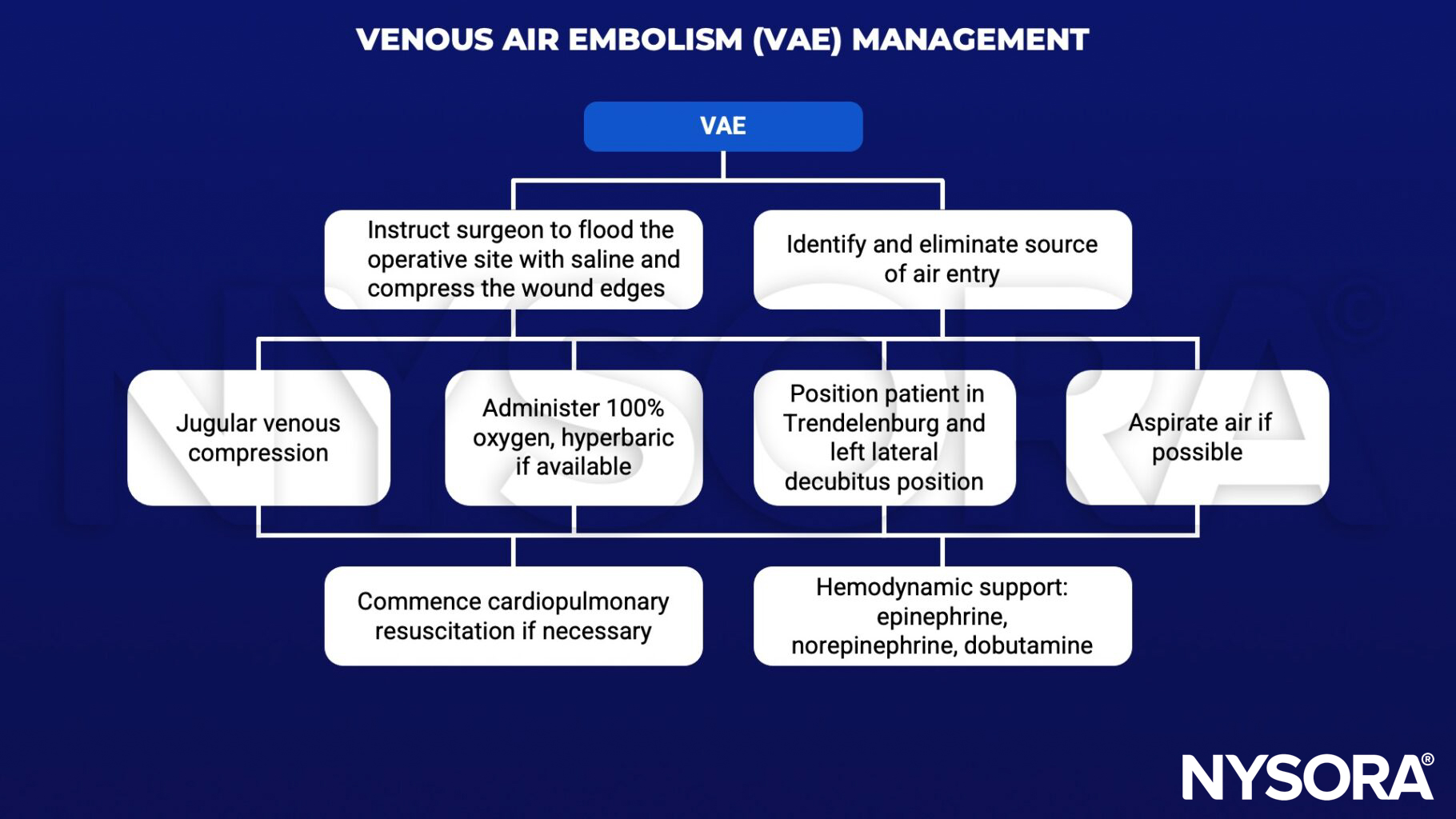
Management
Suggested reading
- Chuang DY, Sundararajan S, Sundararajan VA, Feldman DI, Xiong W. Accidental Air Embolism. Stroke. 2019;50(7):e183-e186.
- McCarthy CJ, Behravesh S, Naidu SG, Oklu R. Air Embolism: Diagnosis, Clinical Management and Outcomes. Diagnostics (Basel). 2017;7(1):5. Published 2017 Jan 17.
- Mirski MA, Lele AV, Fitzsimmons L, Toung TJ. Diagnosis and treatment of vascular air embolism. Anesthesiology. 2007;106(1):164-177.
- Webber S, Andrzejowski J, Francis G. Gas embolism in anaesthesia. BJA CEPD Reviews. 2002;2(2):53-7.