Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About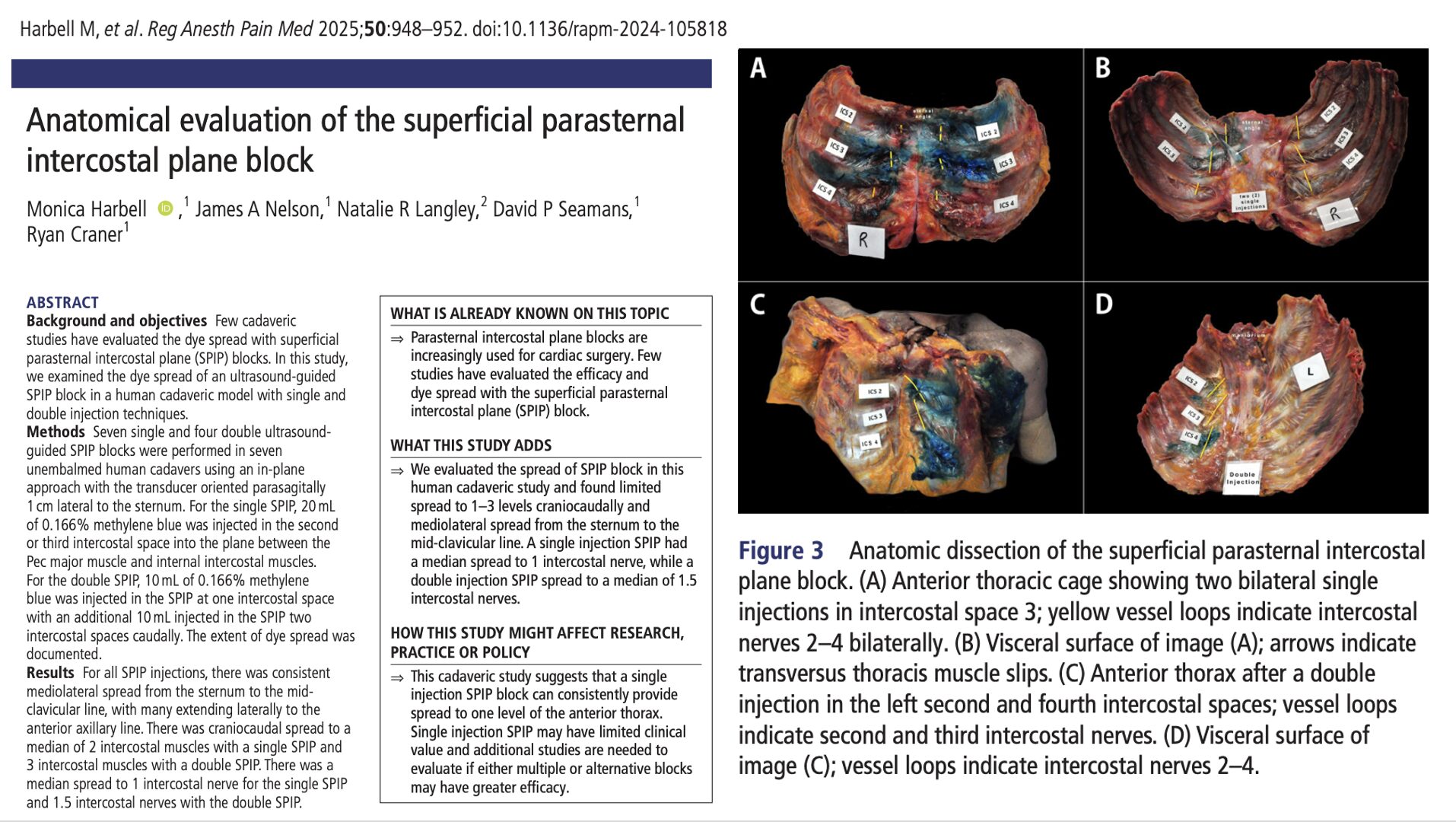





Parasternal intercostal plane blocks have rapidly become staples in modern cardiac anesthesia pathways, especially for sternotomy analgesia, where opioid minimization and stable respiratory mechanics are essential. Among them, the superficial parasternal intercostal plane (SPIP) block has gained attention as a safer alternative to the deep parasternal block (DPIP)—largely because it avoids the internal thoracic artery and is unaffected by tissue disruption during internal mammary harvest. SPIP deposits local anesthetic between the pectoralis major and external intercostal membrane, targeting the anterior cutaneous branches of T2–T6.
Yet despite widespread clinical use, surprisingly little is known about how far the injectate actually spreads along the anterior thoracic wall. Only two small cadaveric studies have previously evaluated SPIP spread, and reported results were limited and variable. This raises a critical question: Can a single-shot SPIP block truly provide meaningful craniocaudal coverage for sternotomy analgesia—or does its spread fall short of what clinicians often assume?
This anatomical cadaveric study directly examined injectate distribution after single and double SPIP injections, using standardized ultrasound-guided technique and methylene blue dye. The researchers quantified mediolateral and craniocaudal spread, as well as dye contact with intercostal nerves—offering rare anatomical insight into the functional coverage clinicians may expect from this block.
Study objective and methods
The primary objective was to characterize the anatomical spread of injectate from ultrasound-guided SPIP blocks—single versus double injections—using cadaveric dissection.
- Design: Anatomical cadaveric study.
- Setting: Mayo Clinic Center for Procedural Innovation (USA).
- Specimens: Seven unembalmed cadavers without prior thoracic surgery.
- SPIP technique: Transducer placed parasagittally 1 cm lateral to the sternum. Needle advanced in-plane into the fascial plane between the pectoralis major and the external intercostal membrane.
- Single SPIP: 20 mL methylene blue injected at the 2nd or 3rd intercostal space.
- Double SPIP: 10 mL at one level plus 10 mL two interspaces caudally (total 20 mL per side).
- Assessments: Full anterior and posterior thoracic dissection to document mediolateral dye spread, craniocaudal spread across the intercostal muscles, and dye presence on the intercostal nerves.
- Primary outcome: Craniocaudal and mediolateral spread patterns for single versus double SPIP.
- Secondary outcomes: Number of intercostal muscles and nerves contacted; variability of distribution.
Key findings
-
Consistent mediolateral spread to the mid-clavicular line
Across all injections, dye spread from the sternum to at least the mid-clavicular line, and in many specimens extended to the anterior axillary line. This demonstrates reliable horizontal distribution of injectate along the superficial plane.
-
Limited craniocaudal spread: 2 levels with single SPIP, 3 with double SPIP
Single injections reached a median of 2 intercostal muscles, while double injections reached 3 levels. This restricted vertical spread suggests a narrower field of coverage than DPIP.
-
Minimal spread to intercostal nerves
Despite acceptable muscle staining, dye contacted only 1 intercostal nerve (median) with single SPIP and 1.5 nerves with double SPIP. The limited neural involvement raises questions about the effectiveness of broad sternotomy analgesia.
-
Double injections improved but did not fully overcome limited nerve coverage
Although double SPIP produced greater craniocaudal spread, staining still fell short of the multi-level coverage typically seen with a single DPIP block.
-
Findings align with previous small studies—SPIP coverage is narrower than commonly assumed
Results confirm prior cadaveric reports demonstrating that SPIP’s spread is modest, variable, and substantially less extensive than DPIP, particularly regarding intercostal nerve involvement.
Conclusion
In this cadaveric model, the SPIP block produced limited and inconsistent craniocaudal spread, reaching only 1–3 intercostal levels and contacting few intercostal nerves. While mediolateral spread was reliable, the restricted vertical extent suggests that a single-injection SPIP may not provide adequate coverage for sternotomy analgesia. Double injections modestly improved spread, but not to the degree typically associated with deep parasternal techniques. Clinical correlation is required to determine whether SPIP should be performed at multiple levels—or whether alternative or combined blocks offer more reliable analgesic coverage.
Future research
- Define optimal injection level(s) and total volumes needed for clinically meaningful coverage.
- Compare SPIP vs DPIP in vivo to clarify relative neural blockade and analgesic quality.
- Evaluate double- and triple-level SPIP strategies in prospective clinical trials.
- Determine whether specific sternotomy subtypes require tailored SPIP patterns.
- Explore ultrasound or contrast-enhanced imaging to map injectate spread in live patients.
Clinical implications
Clinicians should recognize that while the SPIP block is technically simple and avoids the risks associated with deep parasternal approaches, its craniocaudal spread is limited and may cover only a narrow portion of the anterior thorax. For sternotomy analgesia, a single injection may not sufficiently anesthetize multiple intercostal levels, and multi-level injections or alternative blocks may be required. These anatomical findings underscore the need to refine the SPIP technique, tailor injections to surgical requirements, and avoid overestimating coverage based solely on superficial placement.
Clinical pearls
- SPIP spread is reliable mediolaterally but limited vertically (1–3 levels).
- Single SPIP typically reaches only 1 intercostal nerve.
- Double injections provide modest improvement but still limited neural coverage.
- Coverage is substantially less than that seen with DPIP blocks.
Practical tip: Use multi-level SPIP injections when broader anterior thoracic coverage is needed—single shots rarely spread far enough.
For more detailed information, refer to the full article in RAPM.
Harbell M. et al. Anatomical evaluation of the superficial parasternal intercostal plane block. Reg Anesth Pain Med. 2025;50:948-952.
Download the Nerve Blocks App HERE for in-depth insights on the parasternal block. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Module on NYSORA360!