Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About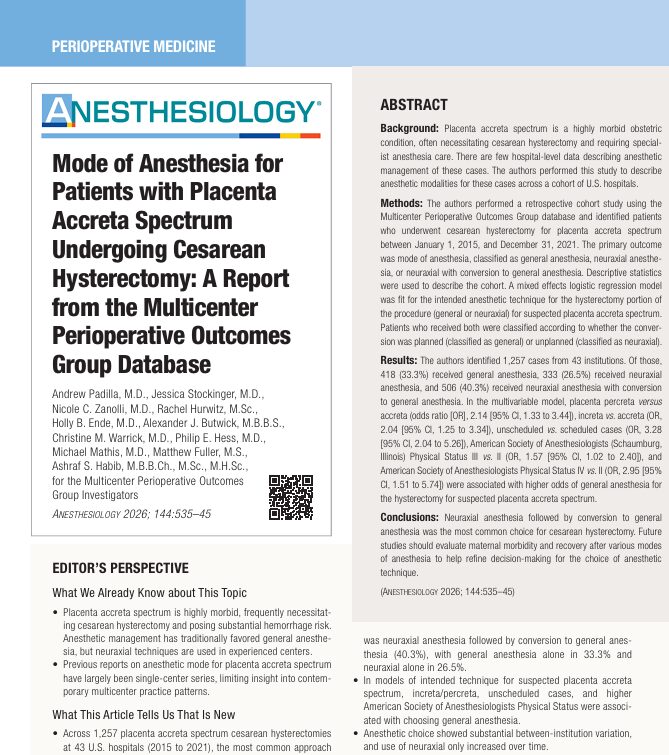





Placenta accreta spectrum (PAS) remains one of the most challenging and high-risk conditions in modern obstetrics. A newly published multicenter study by Padilla et al. (Anesthesiology, 2026) provides critical insights into anesthetic management patterns during cesarean hysterectomy, offering valuable guidance for clinicians navigating this complex scenario.
What is placenta accreta spectrum?
Placenta accreta spectrum refers to abnormal placental adherence or invasion into the uterine wall. It is categorized into three subtypes based on depth of invasion:
- Placenta accreta – superficial adherence to the myometrium
- Placenta increta – invasion into the myometrium
- Placenta percreta – penetration through the uterus, possibly involving adjacent organs
Why it matters
- PAS is associated with massive obstetric hemorrhage
- Frequently requires cesarean hysterectomy
- Carries significant maternal morbidity and mortality
The incidence has risen dramatically, from approximately 1 in 10,000 deliveries in the 1960s to 3.11 per 1,000 deliveries today, largely due to rising cesarean delivery rates.
Study overview: large multicenter analysis
This landmark study analyzed:
- 1,257 patients
- 43 U.S. hospitals
- Timeframe: 2015–2021
The goal was to evaluate real-world anesthesia practices in PAS patients undergoing cesarean hysterectomy.
Key anesthetic modalities studied
- General anesthesia (GA)
- Neuraxial anesthesia (spinal, epidural, combined spinal-epidural)
- Neuraxial anesthesia with conversion to general anesthesia
Major findings: how anesthesia is actually practiced
Distribution of anesthesia techniques
- 40.3% – neuraxial anesthesia with conversion to general anesthesia
- 33.3% – general anesthesia alone
- 26.5% – neuraxial anesthesia alone
The most common approach was combined neuraxial + general anesthesia, typically involving planned or unplanned conversion.
Why does anesthetic choice vary?
-
Severity of placental invasion
Patients with more severe disease were more likely to receive general anesthesia:
- Placenta increta → OR 2.04
- Placenta percreta → OR 2.14
Clinical reasoning:
- Increased risk of hemorrhage
- Longer surgical duration
- Need for rapid airway control and hemodynamic stability
-
Scheduled vs. emergency surgery
- Unscheduled cases had significantly higher odds of general anesthesia (OR 3.28)
Explanation:
- Emergencies often involve active bleeding
- Limited preparation time
- Higher urgency favors rapid induction
-
Patient comorbidity (ASA status)
Higher ASA physical status increased the likelihood of general anesthesia:
- ASA III → OR 1.57
- ASA IV → OR 2.95
This reflects concerns about:
- Physiologic instability
- Risk of intraoperative deterioration
- Need for controlled airway and ventilation
-
Institutional variation
- 37% of variability in anesthetic choice was due to institutional factors
This includes:
- Local protocols
- Availability of expertise
- Surgical team preferences
- Blood management strategies
Neuraxial anesthesia: rising trend
Despite historical preference for general anesthesia, the study highlights a growing shift:
- Neuraxial-only use increased over time
- Some centers increasingly adopt combined or staged approaches
Advantages of neuraxial techniques
- Maternal awareness during delivery
- Reduced airway complications
- Better postoperative analgesia
- Lower neonatal exposure to anesthetic agents
Conversion from neuraxial to general anesthesia
Why conversion occurs
Conversion may be:
Planned
- After fetal delivery
- To facilitate hysterectomy
Unplanned
- Massive hemorrhage
- Inadequate analgesia
- Poor surgical exposure
Key insight
- Over 50% of conversions had unclear documentation
- These cases had higher blood loss and transfusion rates
This suggests many conversions may be reactive to intraoperative complications.
Hemorrhage and transfusion: central challenges
Blood loss
- Median estimated blood loss: 2,000 mL
- Highest in the combined anesthesia group
Transfusion rates
- > 50% received red blood cell transfusion
- Median transfusion volume: 903 mL
Other products:
- Fresh frozen plasma: 28.5%
- Platelets: 12.7%
- Cryoprecipitate: 9.1%
Role of cell salvage
- Used in only 21.2% of cases
Clinical implication:
- Underutilization of cell saver technology
- Potential opportunity to reduce allogeneic transfusion
Step-by-step approach to anesthesia planning in PAS
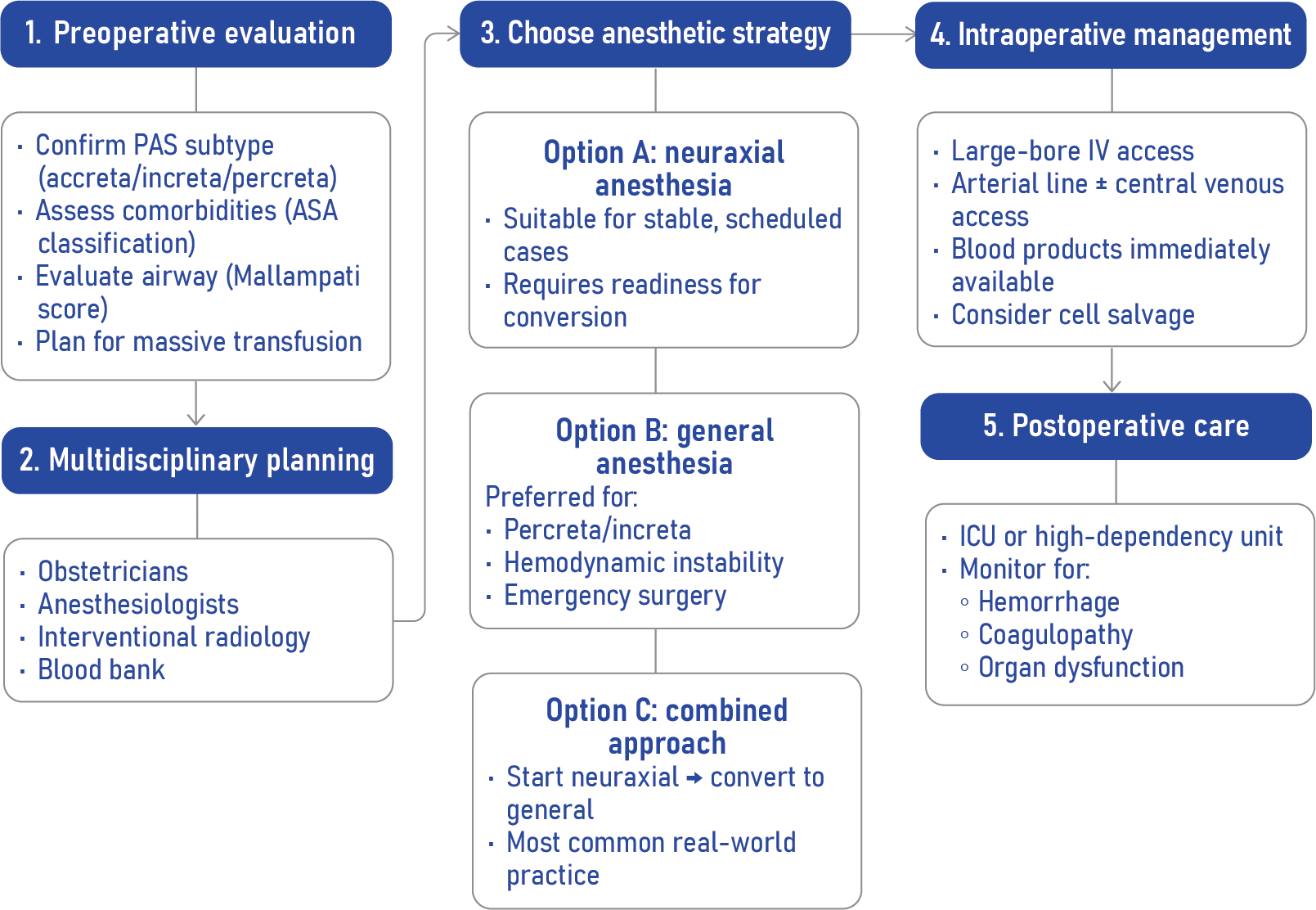
Conclusion
This multicenter study reshapes our understanding of anesthesia in placenta accreta spectrum. The dominance of combined neuraxial and general anesthesia reflects a pragmatic balance between maternal safety and surgical demands.
As PAS incidence continues to rise, anesthesiologists must adopt:
- Flexible strategies
- Evidence-based decision-making
- Strong multidisciplinary coordination
Ultimately, tailoring anesthesia to patient condition, surgical complexity, and institutional expertise remains the cornerstone of optimal care.
Reference: Padilla A et al. Mode of Anesthesia for Patients with Placenta Accreta Spectrum Undergoing Cesarean Hysterectomy: A Report from the Multicenter Perioperative Outcomes Group Database. Anesthesiology. 2026;144:535-545.
For more information and practical flowcharts on placenta accreta, get NYSORA’s Anesthesiology Manual!