Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About



Introduction
The growing prevalence of class III obesity (BMI ≥ 40 kg/m²) is transforming perioperative care worldwide. Patients with obesity present unique respiratory and cardiovascular challenges, particularly during general anesthesia and mechanical ventilation. A 2026 narrative review by Boesing et al. (BJA) highlights the critical role of positive end-expiratory pressure (PEEP) in optimizing outcomes for this high-risk population.
Understanding obesity-related respiratory physiology
Key physiological changes
Obesity significantly alters pulmonary mechanics, increasing the risk of complications during surgery.
- reduced functional residual capacity (FRC)
- increased pleural pressure
- decreased lung compliance
- increased airway resistance
- ventilation–perfusion mismatch
According to the review by Boesing et al., FRC decreases by 5–15% for every 5 kg/m² increase in BMI, leading to early airway closure and alveolar collapse.
Why PEEP matters in obese surgical patients
Role of PEEP in lung protection
PEEP is a cornerstone of lung-protective ventilation. It works by:
- preventing alveolar collapse (atelectasis)
- increasing end-expiratory lung volume (EELV)
- improving oxygenation
- enhancing ventilation–perfusion matching
When applied correctly, PEEP counteracts elevated pleural pressures seen in obesity.
Risks of improper PEEP
However, inappropriate PEEP levels can lead to:
- alveolar overdistension
- increased lung stress and strain
- reduced venous return
- cardiovascular instability
Atelectasis: a major perioperative risk
Why obese patients are vulnerable
Up to 90% of patients under general anesthesia develop atelectasis, with higher rates in obesity.
Contributing factors include:
- increased abdominal pressure pushing the diaphragm upward
- reduced lung volumes
- impaired surfactant function
- high pleural pressures
Clinical consequences
Personalized PEEP: the emerging standard
Why fixed PEEP is insufficient
Traditional fixed PEEP strategies (e.g., 4–12 cm H₂O) often fail to address individual variability.
Studies show:
- many obese patients require PEEP > 15 cm H₂O
- some cases (BMI > 50) may require 20–25 cm H₂O
Benefits of personalized PEEP
- improved respiratory compliance
- reduced driving pressure
- better oxygenation
- decreased atelectasis
Step-by-step PEEP optimization strategy
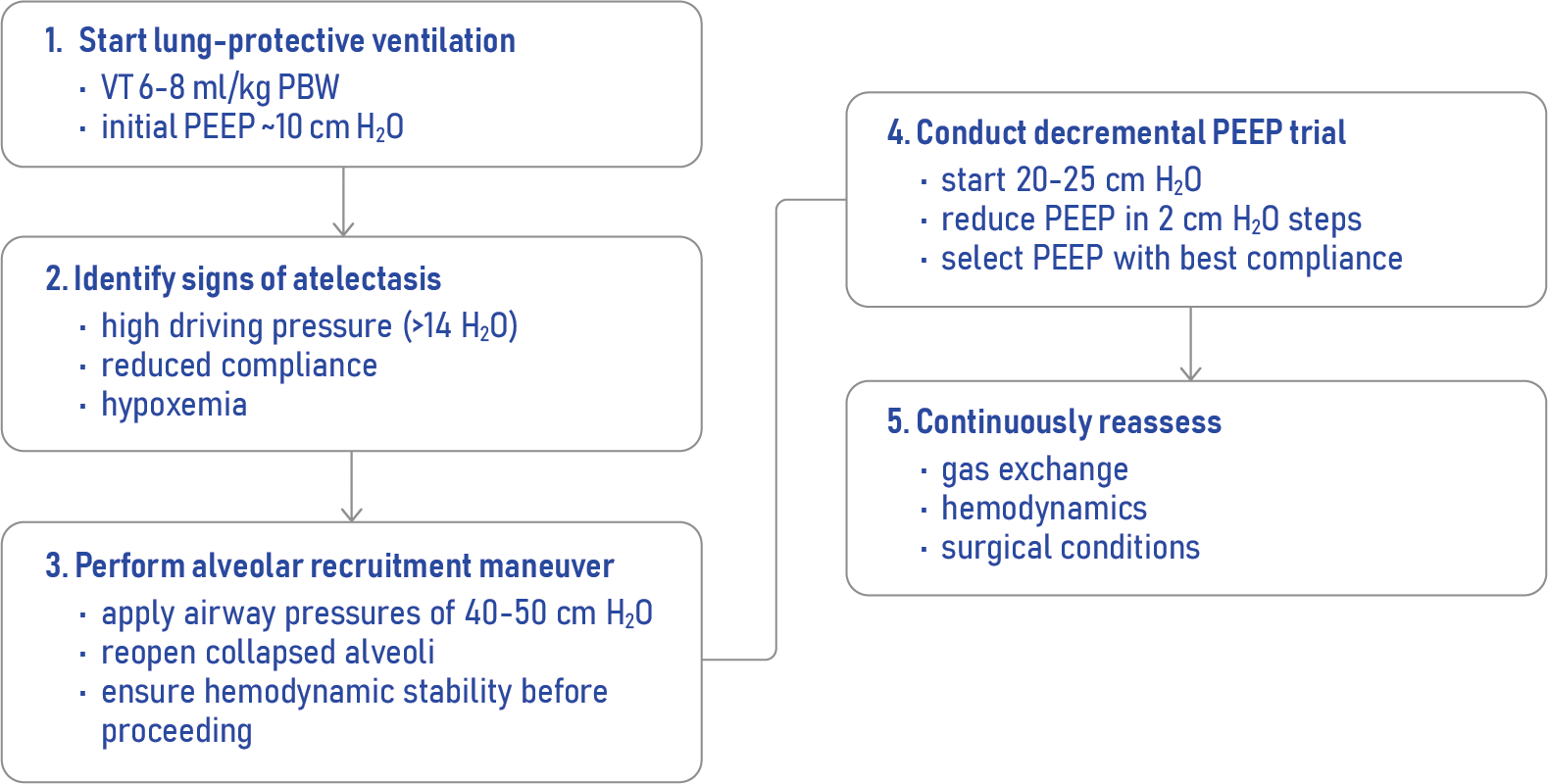
Clinical indicators for PEEP adjustment
- driving pressure > 14 cm H₂O
- decreasing lung compliance
- worsening oxygenation
- increasing FiO₂ requirements
Cardiovascular effects of PEEP
Positive effects
- reduced left ventricular afterload
- improved oxygenation
- decreased pulmonary vascular resistance (with proper use)
Potential adverse effects
- reduced venous return
- hypotension
- bradycardia (especially during recruitment maneuvers)
Interestingly, in obese patients:
- elevated pleural pressures may protect against hemodynamic compromise
- cardiac output often remains stable even at higher PEEP levels
Interplay between lung and heart
PEEP influences:
- cardiac preload
- right ventricular afterload
- pulmonary circulation
Key takeaway:
- balance is essential. Optimize lung function without impairing circulation
Postoperative challenges
Even with optimal intraoperative PEEP:
- benefits may disappear within hours after extubation
- atelectasis can recur quickly
This highlights the need for:
- postoperative respiratory support
- continued lung recruitment strategies
Practical recommendations
Core clinical principles
- anticipate obesity-related physiology
- identify atelectasis risk early
- use recruitment maneuvers cautiously
- personalize PEEP settings
- monitor continuously for complications
Conclusion
PEEP optimization in obese patients undergoing general anesthesia is complex but essential. A personalized, physiology-driven approach offers the best balance between improving respiratory function and maintaining cardiovascular stability.
While current evidence supports individualized strategies, further large-scale studies are needed to confirm their impact on patient-centered outcomes.
Reference: Boesing C et al. Positive end-expiratory pressure optimisation during general anaesthesia in patients with obesity: a narrative review of respiratory and cardiovascular outcomes. Br J Anaesth. 2026;136:970-982.
For real-time clinical educational support, dosing information, and case simulations, explore the NYSORA Anesthesia Assistant App.