Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About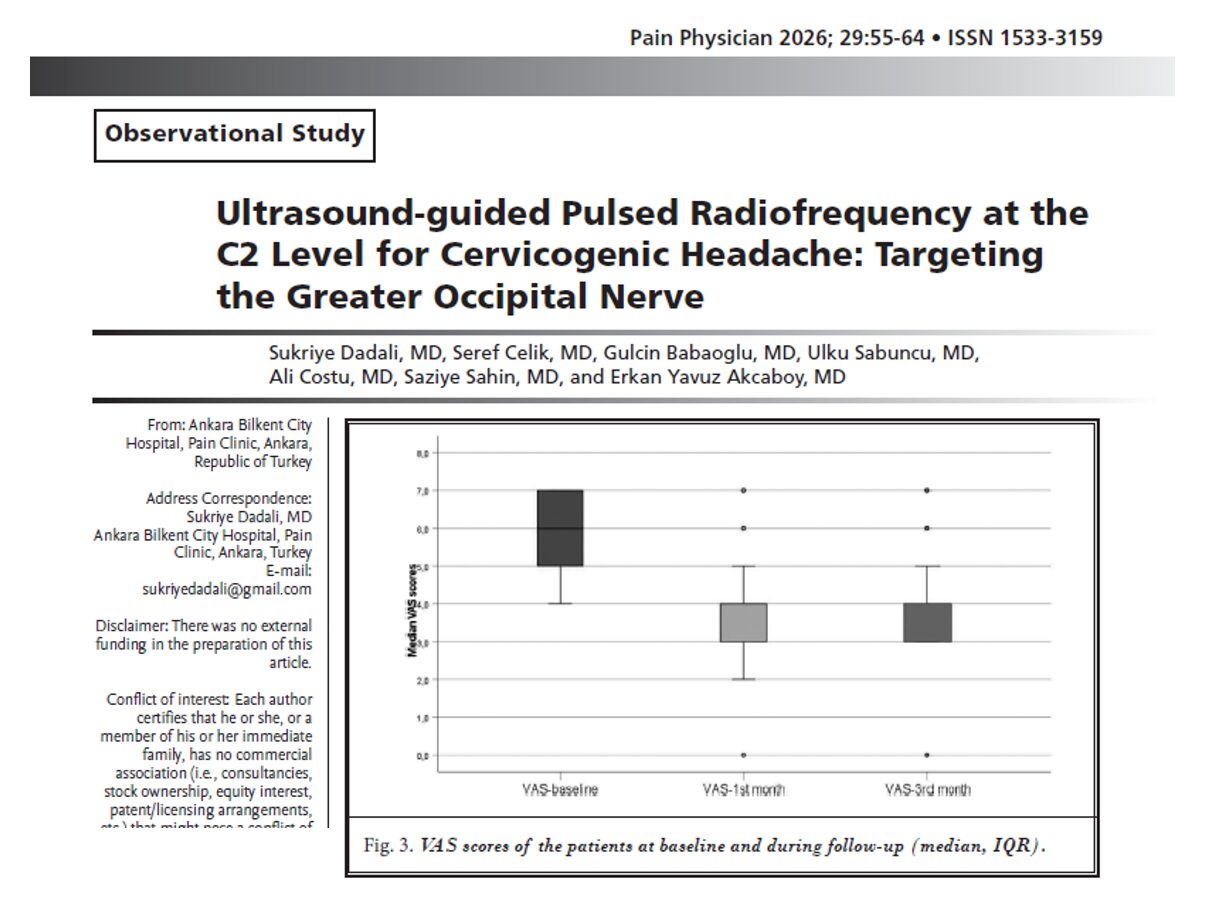





Cervicogenic headache (CHA) is a secondary headache disorder originating from dysfunction in the cervical spine and its associated structures. Often presenting as unilateral occipital pain radiating toward the frontal region, CHA is frequently accompanied by neck pain, reduced cervical mobility, and significant functional impairment. Despite multimodal treatment approaches, many patients remain refractory to pharmacologic therapy, prompting increasing interest in interventional pain techniques.
A recent prospective observational study by Dadali et al., published in Pain Physician, evaluates the efficacy and safety of ultrasound-guided pulsed radiofrequency (PRF) applied to the greater occipital nerve (GON) at the C2 vertebral level, demonstrating meaningful improvements in pain intensity, frequency, and analgesic use.
Understanding cervicogenic headache
CHA is estimated to account for approximately 15–20% of chronic headache cases and is classified as a secondary headache disorder arising from cervical spine pathology.
key clinical characteristics include:
- Unilateral, non-throbbing occipital pain
- Radiation to frontal, orbital, or contralateral regions
- Associated neck pain and stiffness
- Triggering by neck movement or sustained posture
The underlying mechanism involves convergence of cervical (C1–C3) and trigeminal sensory pathways, explaining the referral of pain from the neck to the head.
Limitations of conventional management
Standard CHA treatment includes:
- Pharmacologic therapy (NSAIDs, analgesics)
- Physical therapy and rehabilitation
- Behavioral and supportive strategies
However, limitations include:
- Incomplete pain relief
- Frequent recurrence
- Medication overuse
- Persistent functional impairment
These challenges highlight the need for targeted interventional approaches.
Greater occipital nerve: a key therapeutic target
The greater occipital nerve (GON), arising from the dorsal ramus of C2, plays a central role in cervicogenic headache pathophysiology.
Why target the GON?
- Direct involvement in occipital pain transmission
- Functional connection with trigeminocervical complex
- Accessibility for ultrasound-guided interventions
Diagnostic GON blocks are commonly used to confirm the source of pain and predict response to further treatment.
Pulsed radiofrequency: neuromodulation without destruction
Pulsed radiofrequency is a minimally invasive technique that delivers intermittent electrical energy to neural tissue.
Key advantages:
- Modulates pain signaling without nerve destruction
- Preserves neural integrity
- Reduces risk compared to continuous radiofrequency ablation
Mechanistically, PRF alters synaptic transmission and neurotransmitter activity, leading to reduced nociceptive signaling.
Study design and patient selection
The study included patients diagnosed with cervicogenic headache who met strict clinical criteria.
key aspects:
- 51 patients screened
- 34 responded to diagnostic GON block
- 32 patients completed PRF treatment and follow-up
Only patients achieving ≥ 50% pain relief after diagnostic block proceeded to PRF, emphasizing the importance of patient selection.
Procedure technique
The intervention was performed under ultrasound guidance to ensure accuracy and safety.
procedural steps:
- Patient positioned prone with neck flexed
- Identification of C2 landmarks and surrounding muscles
- Visualization of GON between:
- Obliquus capitis inferior muscle
- Semispinalis capitis muscle
PRF parameters:
- Voltage: 45 V
- Frequency: 5 Hz
- Pulse width: 5 ms
- Temperature: ≤ 42°C
- Duration: 360 seconds
Clinical outcomes: significant and sustained improvements
1. Reduction in pain intensity
- Baseline VAS ≈ 6
- Reduced to ≈ 4 at 1 and 3 months
2. decreased headache frequency
- Headache days reduced from ~20/month to ~6/month
3. shorter headache duration
- Reduced from ~6.5 hours to ~3 hours per episode
4. reduced analgesic use
- Significant decrease in medication days per month
- Slight increase at 3 months but still below baseline
These findings are supported by the table on page 8, which summarizes consistent improvements across all clinical parameters .
Safety profile
The procedure demonstrated a favorable safety profile.
Observed effects:
- No serious complications
- Mild, transient side effects in ~22% of patients:
- Dizziness
- Nausea
- Drowsiness
These effects resolved without intervention.
Clinical importance:
- Confirms diagnosis
- Identifies responders
- Improves treatment success rates
Patients with ≥ 50% pain relief after diagnostic block were significantly more likely to benefit from PRF.
Clinical implications
This study reinforces several key principles:
- Ultrasound guidance enhances procedural accuracy
- PRF offers a safe neuromodulatory alternative to destructive techniques
- Targeted nerve interventions can reduce reliance on systemic medications
- Early identification of responders improves outcomes
Additionally, the findings support integration of PRF into multimodal pain management pathways for cervicogenic headache.
Limitations and future directions
Despite promising results, limitations include:
- Small sample size
- Single-center design
- Short follow-up duration (3 months)
- Coexistence of migraine in some patients
Future research should focus on:
- Long-term efficacy
- Comparative studies with other interventional techniques
- Optimization of PRF protocols
Conclusion
Ultrasound-guided pulsed radiofrequency targeting the greater occipital nerve at the C2 level represents an effective and safe treatment option for cervicogenic headache. By significantly reducing pain intensity, frequency, and medication use, this technique offers a valuable addition to interventional pain management strategies.
As evidence continues to evolve, PRF may become a cornerstone therapy for patients with refractory cervicogenic headache, particularly when guided by diagnostic nerve block response.
For more information, refer to the full article in Pain Physician.
Dadali S, Celik S, Babaoglu G, et al. Ultrasound-guided Pulsed Radiofrequency at the C2 Level for Cervicogenic Headache: Targeting the Greater Occipital Nerve. Pain Physician. 2026;29(1):55-64.
For a detailed guide on ultrasound-guided greater occipital nerve blocks, get your copy of NYSORA’s Ultrasound-Guided Interventional Pain Procedures Manual!