Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About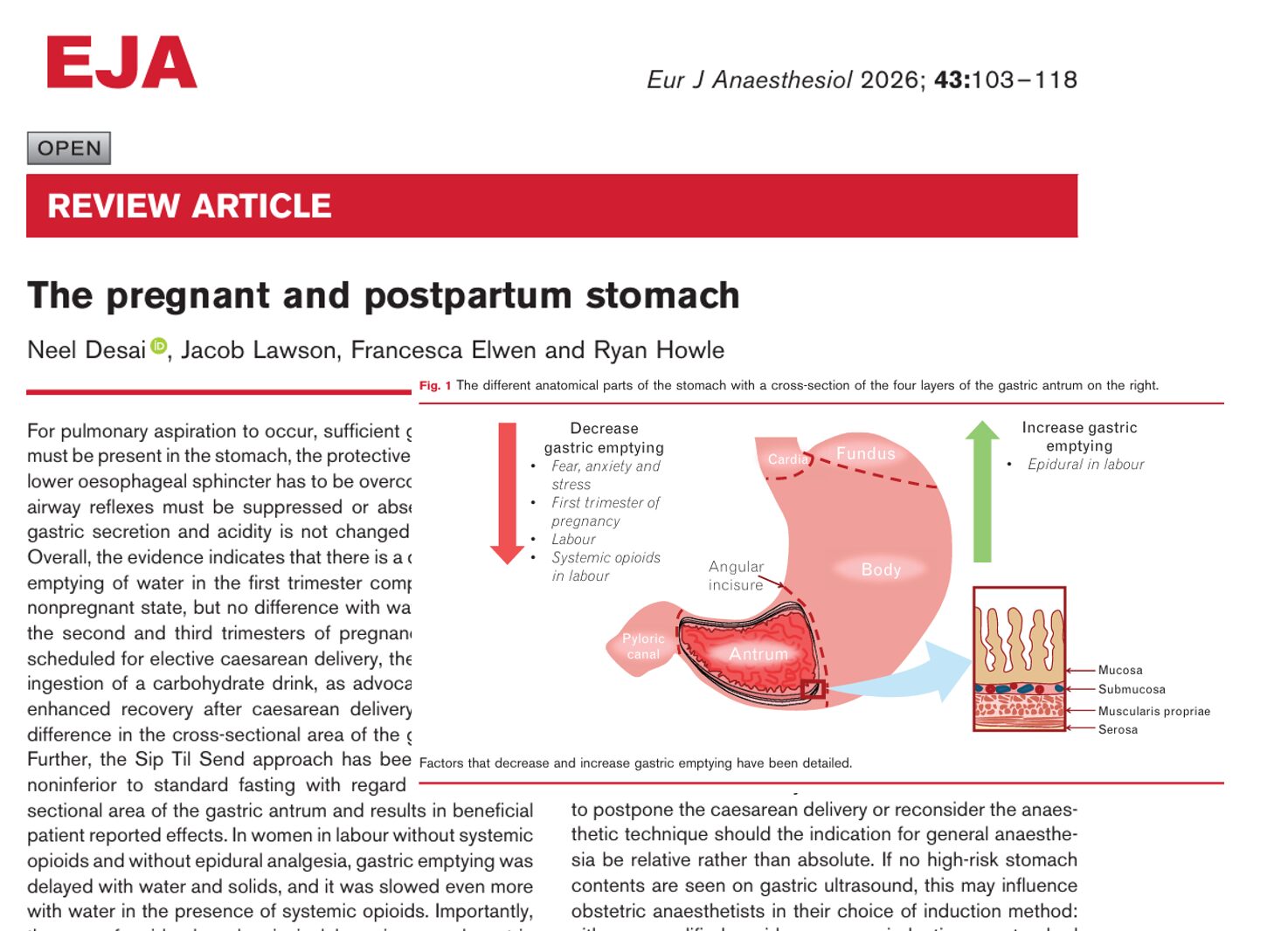





Introduction
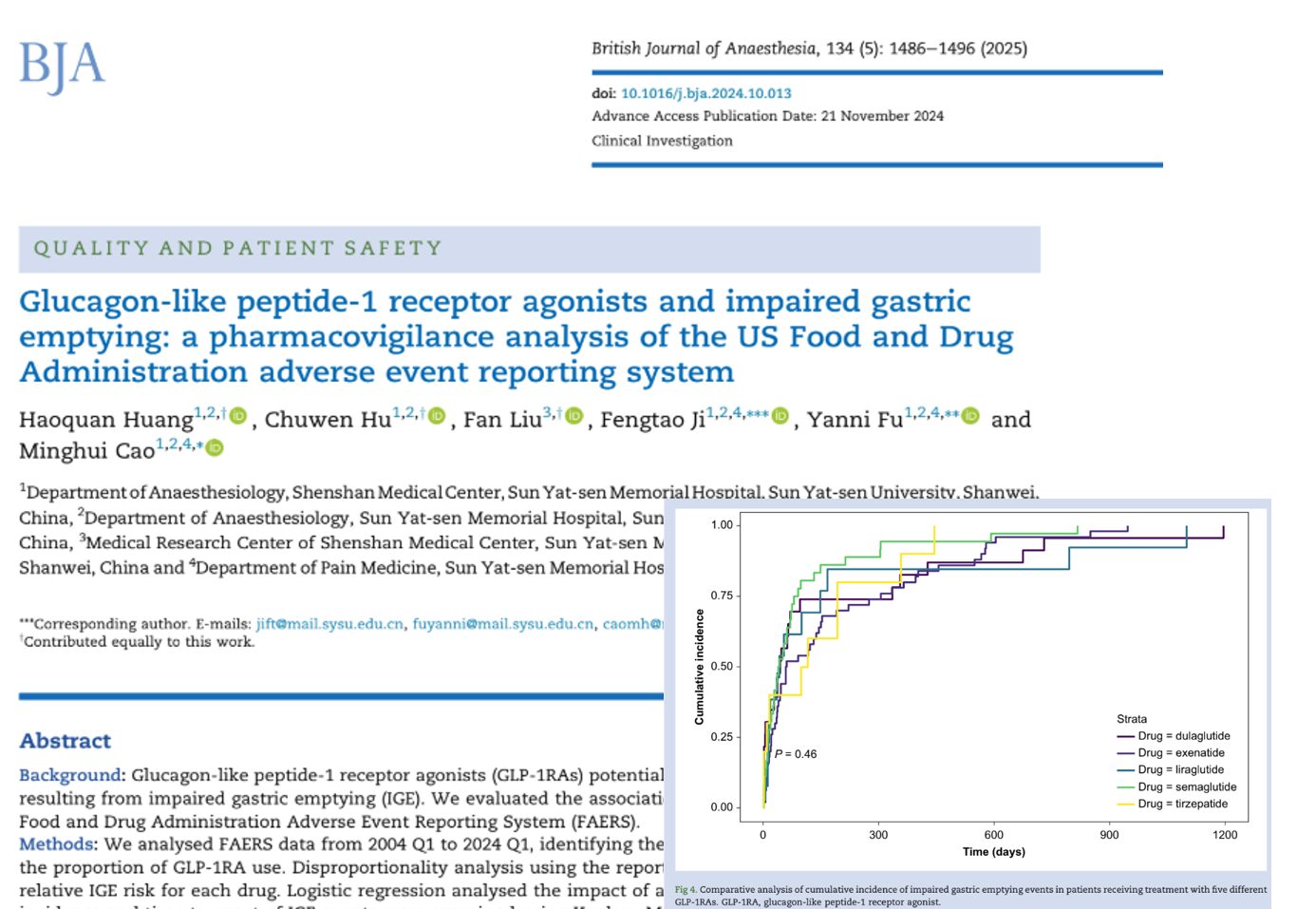
Pulmonary aspiration remains one of the most feared complications in obstetric anesthesia. Although rare, it carries significant maternal and neonatal morbidity. A comprehensive 2026 review published in the European Journal of Anaesthesiology provides updated insights into gastric physiology during pregnancy, labor, and the postpartum period, along with the evolving role of gastric ultrasound.
Anatomy and physiology of the stomach
The stomach is a distensible muscular organ divided into four main regions:
- Cardia
- Fundus
- Body
- Pylorus
Its primary physiological roles include:
- Temporary storage of food and fluids
- Mechanical and chemical digestion
- Regulation of gastric emptying into the duodenum
- Secretion of intrinsic factor
- Modulation of appetite and satiety
Key physiological insight
- Basal gastric acid secretion and acidity do not change during pregnancy
What causes pulmonary aspiration?
For aspiration to occur, three conditions must be met:
- Presence of sufficient gastric contents
- Reduced lower oesophageal sphincter (LOS) tone
- Suppressed airway reflexes
Pregnancy-specific changes
- LOS pressure decreases progressively, reaching a nadir at ~36 weeks
- Intragastric pressure increases due to the gravid uterus
- Risk increases significantly under general anesthesia
Gastric emptying during pregnancy
First trimester
- Gastric emptying of liquids is delayed
- Likely influenced by hormonal changes and early pregnancy physiology
Second and third trimesters
- No significant difference in gastric emptying for:
- Liquids
- Solids
Clinical takeaway
- Early pregnancy poses a higher risk of delayed gastric emptying than later stages
Gastric emptying during labor
Labor significantly alters gastric physiology.
Without analgesia or opioids
- Gastric emptying is delayed for both liquids and solids
With systemic opioids
- Further slowing of gastric emptying
With epidural analgesia
- Gastric emptying improves
- However, it does not return to nonpregnant levels
Postpartum gastric physiology
- Gastric emptying returns to nonpregnant baseline levels
- No significant differences observed within the first 5 days postpartum
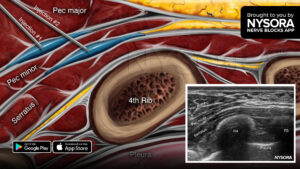
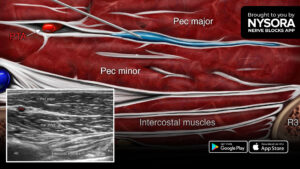
Gastric ultrasound: a game-changing tool
Gastric ultrasound has become a critical bedside tool in obstetric anesthesia.
Why it matters
- Identifies:
- Empty stomach
- Fluid-filled stomach
- Solid contents
- Estimates gastric volume
- Guides anesthesia decisions
How gastric ultrasound works (I-AIM framework)
1. Indication
- Elective cesarean delivery under general anesthesia
- Emergency cesarean when feasible
2. Acquisition
- Positions:
- First trimester/postpartum: supine + right lateral
- Later pregnancy: semirecumbent + right lateral semirecumbent
3. Interpretation
- Empty: collapsed antrum
- Fluids: anechoic/hypoechoic
- Solids: hyperechoic, heterogeneous
4. Medical management
- Adjust anesthesia technique
- Delay surgery if necessary
- Optimize airway strategy
Ultrasound appearances of gastric contents
Empty stomach
- Collapsed, “bull’s eye” appearance
- Grade 0 (safe)
Fluid-filled stomach
- Dilated antrum
- “Starry night” appearance due to air bubbles
- Grade 1–2
Solid contents
- “Frosted glass” appearance
- Indicates high aspiration risk
- Grade 3 (full stomach)
Quantifying gastric volume
A commonly used threshold:
- > 1.5 mL/kg = full stomach (high risk)
Ultrasound indicators of a full stomach:
- Cross-sectional area:
- 608 mm² (semirecumbent)
- 719 mm² (right lateral)
- 960 mm² (right lateral semirecumbent)
- 608 mm² (semirecumbent)
Fasting guidelines in obstetrics
Standard recommendations
- Clear fluids: up to 2 hours
- Solids: 6–8 hours
In labor
- Clear fluids: generally safe
- Solids: remain controversial
Modern approaches: “Sip til send”
A newer approach allows:
- Small sips of water until surgery
Benefits
- Reduced:
- Thirst
- Anxiety
- Nausea
Safety
- No increase in gastric volume observed
- No increase in aspiration risk in studied populations
Clinical implications
For anesthesiologists
- Gastric ultrasound improves decision-making
- Helps tailor airway management strategies
For obstetricians
- Supports safer timing of cesarean delivery
For patients
- May reduce unnecessary prolonged fasting
- Improves comfort and outcomes
Key takeaways
- Gastric physiology changes dynamically across pregnancy stages
- Labor significantly delays gastric emptying
- Clear fluids are generally safe, solids are not
- Gastric ultrasound is transforming obstetric anesthesia practice
- Individual risk assessment is essential
Conclusion
Understanding the pregnant and postpartum stomach is essential for improving maternal safety. While traditional fasting rules remain important, modern tools like gastric ultrasound allow for more individualized and evidence-based care.
As research continues to evolve, the integration of physiology, imaging, and clinical judgment will remain the cornerstone of safe obstetric anesthesia.
Reference: Desai N et al. The pregnant and postpartum stomach. Eur J Anaesthesiol. 2026;43:103-118.
For real-time assessment of gastric contents and practical bedside decision-making, explore the NYSORA POCUS App.