Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the pathophysiology and possible complications of epiglottitis
- Diagnose epiglottitis
- Manage patients with (suspected) epiglottitis
Background
- Epiglottitis is a life-threatening inflammatory condition that causes swelling of the upper airways which can lead to asphyxia and respiratory arrest
- Usually caused by infection
- Noninfectious causes: Trauma from foreign objects, inhalation, and chemical burns
- Affects the epiglottis and nearby structures (arytenoids, aryepiglottic folds, vallecula)
- Symptoms can be exacerbated by patient discomfort or agitation
Pathophysiology
- The airway in the pediatric population differs from adults
- The epiglottis is located more superiorly and anteriorly
- More oblique angle with the trachea
- The narrowest part of the pediatric airway is the subglottis, in contrast to the glottis in adults
- The infant epiglottis is comprised of cartilage and far more pliant
- Infectious processes that lead to edema and mass increase of the epiglottis are more likely to cause symptoms in children
- Each inspiration pulls the edematous epiglottis over the laryngeal airway, causing symptoms
Complications
- Cellulitis
- Cervical adenitis
- Death
- Empyema
- Epiglottic abscess
- Hypoxia
- Meningitis
- Pneumonia
- Pneumothorax
- Prolonged ventilation
- Pulmonary edema
- Respiratory failure
- Sepsis
- Septic arthritis
- Septic shock
- Tracheostomy
- Vocal cord granuloma
- Ludwig angina-type submental infection
Signs & symptoms
- Sudden onset
- Fever
- (Severe) sore throat
- Difficulty swallowing
- Hypersalivation
- Stridor
- “Tripod position”
- Inability to lie flat
- Voice changes
- Dysphagia
- Anxiety
- Tachypnea
- Cyanosis
Diagnosis
- Oropharyngeal exam may lead to loss of airway
- Lateral neck radiograph: Swelling of the epiglottis (only perform in stable, cooperative patients)
- When epiglottitis is suspected, transfer the patient to the operating room for airway assessment
- Differential diagnosis: laryngotracheobronchitis (croup), airway obstruction from a foreign object, acute angioedema, caustic ingestion, diphtheria, peritonsillar/retropharyngeal abscess
Management
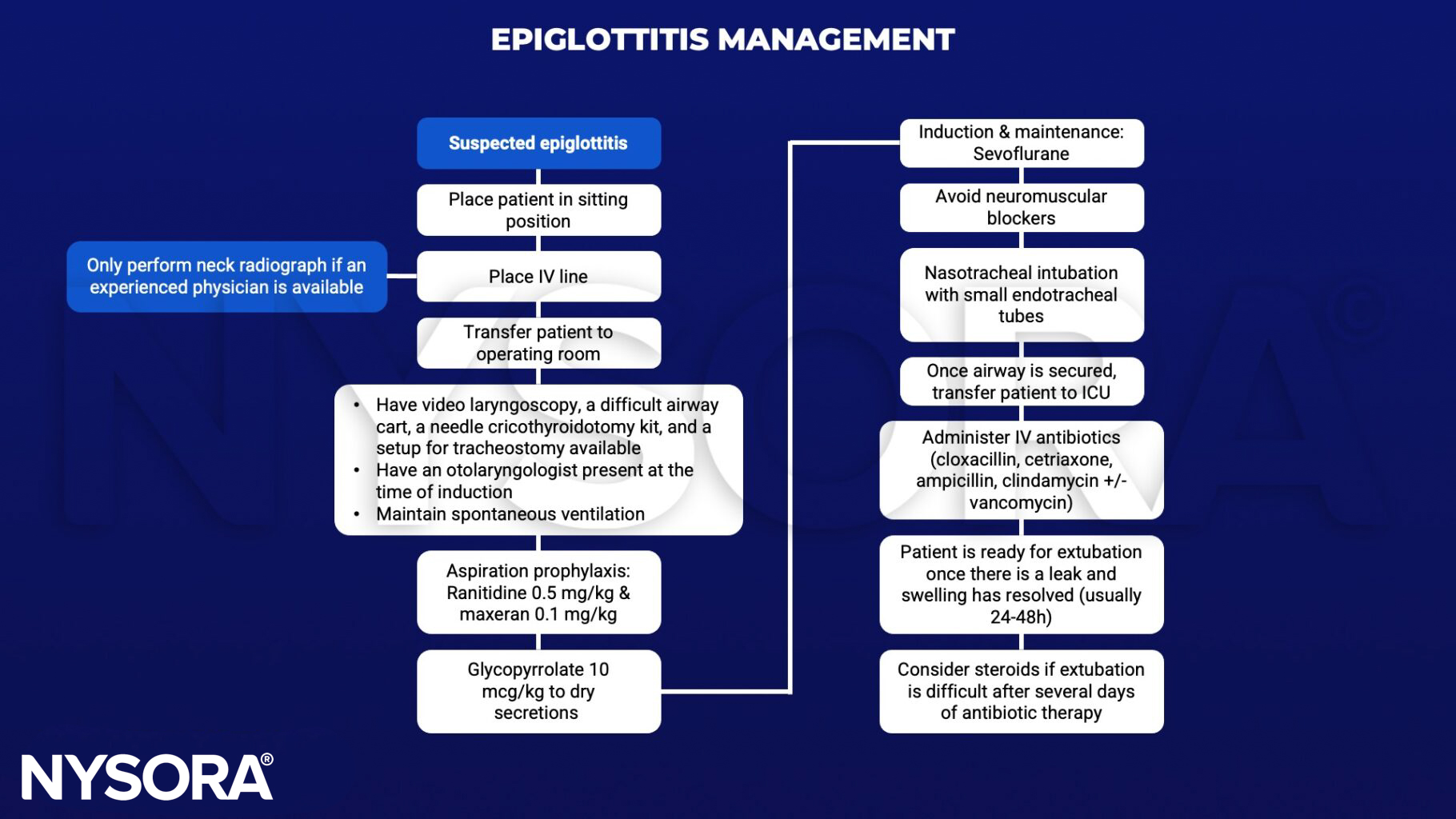
Keep in mind
- Do not agitate the patient
- Be prepared for sudden worsening of the clinical condition
- Oral exams may lead to loss of airway
Suggested reading
- Guerra AM, Waseem M. Epiglottitis. [Updated 2022 Oct 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430960/
- Lichtor JL, Roche Rodriguez M, Aaronson NL, Spock T, Goodman TR, Baum ED. Epiglottitis: It Hasn’t Gone Away. Anesthesiology. 2016;124(6):1404-7.