
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the causes of and risk factors for increased intracranial pressure
- Identify increased intracranial pressure
- Manage increased intracranial pressure
Background
- Increased intracranial pressure (ICP) commonly occurs in patients with traumatic brain injury and subarachnoid hemorrhage
- It is the most frequent cause of morbidity and mortality in these patients
- Brain tumors can also increase ICP
- Increased ICP can impair cerebral perfusion pressure, cerebral blood flow, and cerebral oxygenation, resulting in ischemia, edema, and further increases in ICP
- Can impede surgical access to deep lesions requiring brain retraction
- Can predispose to or exacerbate brain retraction injury
- Can complicate dural closure
Signs
- Before craniotomy:
- Hypertension
- Bradycardia
- Irregular respiratory pattern (Cushing reflex)
- After craniotomy:
- Tense dura
- Brain swelling out of the dural opening
- Difficult brain retraction
- Quantitative measurements:
- ICP monitoring (External ventricular drain, intraparenchymal pressure monitor)
- ICP measurement (Pressure transducer slid into the epidural space from a burr hole or at the edge of a craniotomy)
Risk factors
- Subdural ICP >10 mmHg
- Peritumoral edema
- Mean arterial blood pressure >140 mmHg
- Intraoperative hypotension with systolic blood pressure <90 mmHg
- Glioblastoma
- Metastasis
Causes
- Intracranial
- Tumor
- Infarct
- Trauma
- Hemorrhage
- Hydrocephalus
- abscess/infection
- Parenchymal edema
- Idiopathic
- Extracranial
- Airway obstruction
- Hypoxia/hypercarbia
- Hypertension exceeding cerebral autoregulatory capacity
- Hypotension causing cerebral hypoperfusion and reflex vasodilation
- Venous hypertension from outflow obstruction
- Volatile anesthetics
- Nitroglycerin
- Sodium nitroprusside
- Vomiting, coughing, pain, shivering, and seizure activity during awake craniotomy
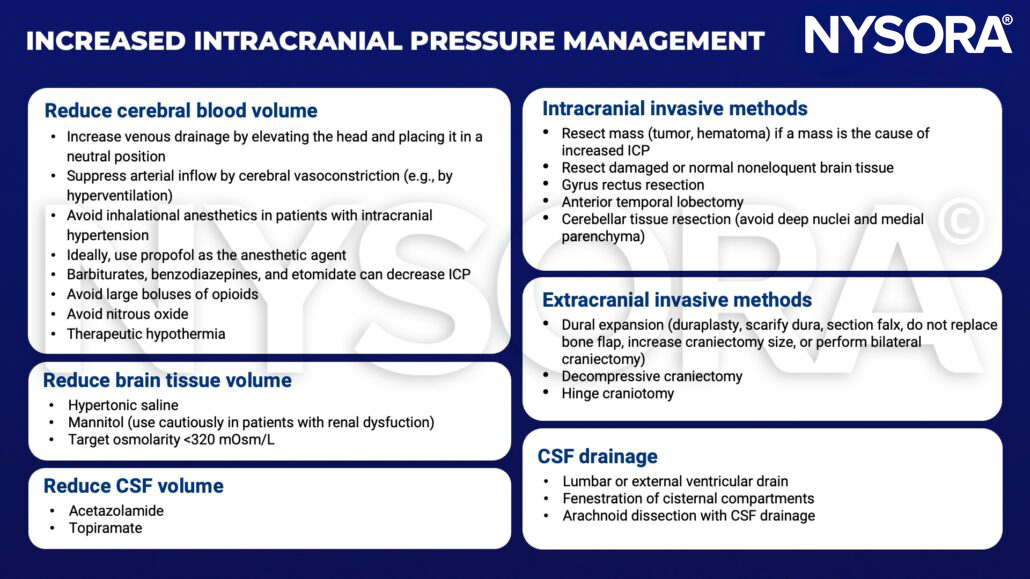
Management
Suggested reading
- Desai VR, Sadrameli SS, Hoppe S, Lee JJ, Jenson A, Steele WJ, et al. Contemporary Management of Increased Intraoperative Intracranial Pressure: Evidence-Based Anesthetic and Surgical Review. World Neurosurgery. 2019;129:120-9.
- Ragland J, Lee K. Critical Care Management and Monitoring of Intracranial Pressure. J Neurocrit Care. 2016;9(2):105-12.
- Tameem A, Krovvidi H. Cerebral physiology. Continuing Education in Anaesthesia Critical Care & Pain. 2013;13(4):113-8.
Clinical updates
Diz et al. (Anesthesia & Analgesia, 2025) report in a meta-analysis of 15 RCTs (>35,000 patients) that balanced crystalloids are associated with higher mortality in traumatic brain injury, likely related to increased cerebral edema and intracranial pressure, whereas non-TBI patients benefited from balanced solutions. These findings support preferential use of normal saline in patients at risk of elevated ICP, reinforcing diagnosis-specific fluid selection in neurocritical care.
- Read more about this study HERE.












