Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About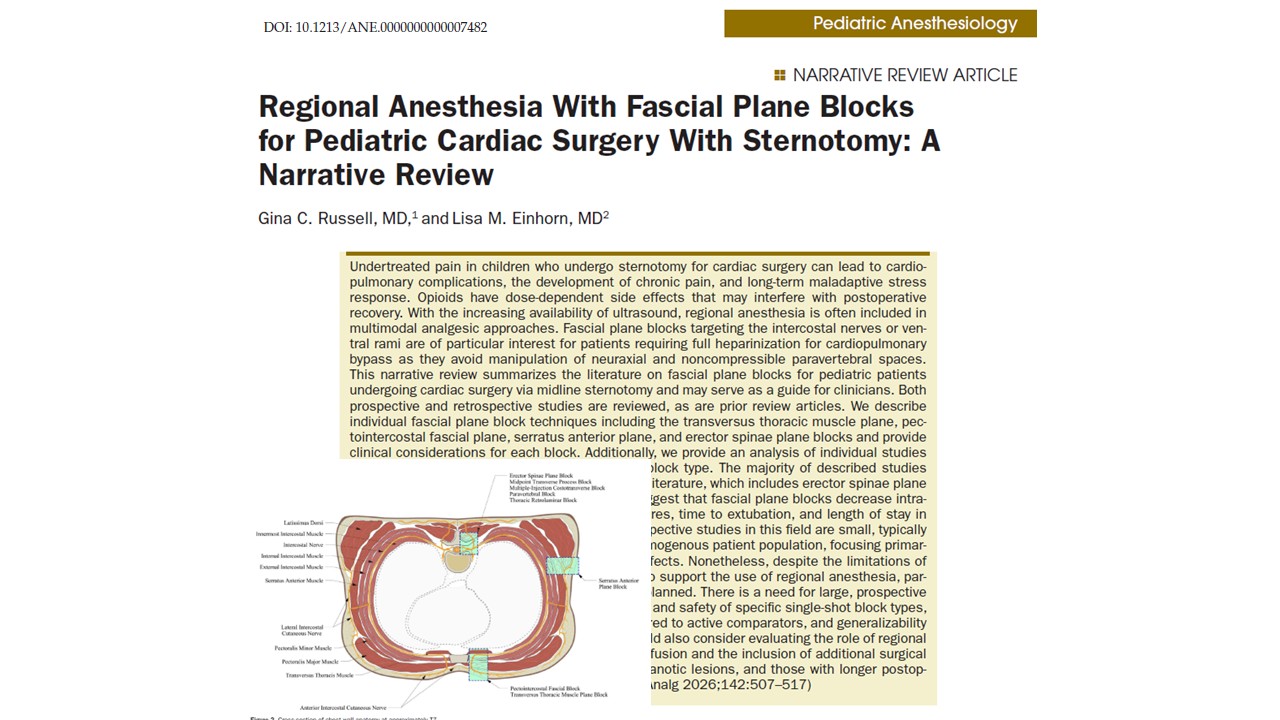





Effective postoperative pain control is a critical component of perioperative care in children undergoing cardiac surgery. Many pediatric cardiac procedures require a median sternotomy, a surgical approach that can produce significant nociceptive and neuropathic pain due to tissue dissection, rib retraction, sternal splitting, and placement of chest drains. Inadequate analgesia in this setting is not simply uncomfortable for the patient—it can contribute to physiologic instability and prolonged recovery.
Pain that is poorly controlled after pediatric cardiac surgery has been associated with increased sympathetic activation, systemic hypertension, pulmonary hypertension, arrhythmias, and ventilator dyssynchrony. These complications may prolong mechanical ventilation and increase the length of stay in the intensive care unit (ICU). Furthermore, persistent poststernotomy pain and negative intensive care experiences may lead to chronic pain syndromes or long-term psychological stress responses in children.
Historically, postoperative analgesia for pediatric cardiac surgery relied heavily on systemic opioids. While opioids remain effective analgesics, they are associated with well-recognized dose-dependent adverse effects. Respiratory depression, nausea, vomiting, ileus, and delayed extubation can complicate postoperative recovery. Prolonged opioid exposure may also lead to tolerance, dependence, or withdrawal symptoms in pediatric patients receiving continuous infusions for several days.
Over the past decade, the increased availability of ultrasound-guided regional anesthesia has transformed perioperative pain management strategies. Fascial plane blocks in particular have gained attention because they provide targeted analgesia while maintaining a favorable safety profile in anticoagulated patients undergoing cardiopulmonary bypass. These techniques avoid the neuraxial and paravertebral spaces, reducing the risk of catastrophic hematoma formation.
This growing interest has led clinicians to explore the use of fascial plane blocks as part of multimodal analgesia protocols for pediatric cardiac surgery. Recent studies suggest that these blocks may significantly reduce opioid requirements, improve postoperative recovery, and support enhanced recovery pathways.
The challenge of poststernotomy pain in children
Median sternotomy involves extensive disruption of the anterior chest wall structures. The sternum is primarily innervated by the anterior cutaneous branches of the intercostal nerves arising from thoracic spinal segments T2 through T6. These nerves originate from the ventral rami of thoracic spinal nerves and travel between layers of the intercostal muscles before emerging near the sternum to supply the anterior chest wall.
In addition to nociceptive input from the incision itself, several other sources contribute to postoperative pain after sternotomy:
- Rib retraction during surgical exposure
- Tissue dissection and muscular trauma
- Chest tubes and mediastinal drains
- Visceral inflammation
- Peripheral nerve irritation or injury
These diverse sources of pain highlight the importance of a multimodal analgesic approach that targets both superficial and deeper thoracic structures.
Traditionally, systemic opioids have been used as the primary analgesic modality. However, excessive opioid use can impair recovery by delaying extubation and increasing respiratory complications. For pediatric cardiac patients, early extubation and fast-track recovery protocols are increasingly prioritized to improve outcomes and reduce ICU stay.
Regional anesthesia techniques, therefore, provide a valuable strategy for achieving effective analgesia while minimizing opioid exposure.
The rise of fascial plane blocks in pediatric cardiac anesthesia
Fascial plane blocks represent a relatively recent development in regional anesthesia. These techniques rely on the injection of local anesthetic into anatomical planes between muscle layers. The injected solution spreads along the fascial planes to reach targeted nerve branches.
The popularity of these blocks has increased significantly with the widespread adoption of ultrasound guidance. Ultrasound allows clinicians to visualize muscles, fascial layers, blood vessels, and pleural structures, improving both safety and accuracy.
One key advantage of fascial plane blocks is their compatibility with the anticoagulation protocols required for cardiopulmonary bypass. Because these blocks avoid the neuraxial and paravertebral spaces, they are considered safer in patients who require full heparinization during cardiac surgery.
Several chest wall fascial plane blocks have been described for pediatric sternotomy analgesia, including:
- Transversus thoracic muscle plane block
- Pectointercostal fascial block
- Serratus anterior plane block
- Erector spinae plane block
These techniques target different branches of the intercostal nerves and thoracic spinal nerves, allowing clinicians to tailor analgesia to the surgical anatomy.
Anterior fascial plane block techniques
Anterior chest wall blocks are commonly used in pediatric cardiac surgery because they can be performed with the patient in the supine position, which is standard surgical positioning for sternotomy. These blocks can be administered either before incision or after surgical closure.
Transversus thoracic muscle plane block
The transversus thoracic muscle plane block (TTMPB) is designed to anesthetize the anterior branches of the intercostal nerves from T2 to T6, which provide sensory innervation to the sternum and adjacent structures.
This block is performed by injecting local anesthetic between the innermost intercostal muscle and the transversus thoracic muscle, a deeper muscle layer located along the posterior surface of the sternum.
One advantage of this approach is the ability of local anesthetics to spread cranially and caudally along the fascial plane, producing multilevel analgesia across the sternotomy incision.
However, the TTMPB also has limitations. The injection plane lies close to important structures, including the internal mammary artery, pleura, and pericardium, thereby increasing technical complexity and requiring careful ultrasound guidance.
Pectointercostal fascial block
The pectointercostal fascial block (PIFB), also referred to as the superficial parasternal block, targets the same anterior cutaneous branches of the intercostal nerves but at a more superficial location.
In this technique, a local anesthetic is injected between the pectoralis major muscle and the intercostal muscles near the sternum.
Because the injection plane is more superficial and relatively free of major vascular structures, the PIFB is generally considered safer and easier to perform compared with deeper parasternal blocks.
The main drawback of the PIFB is the more limited spread of local anesthetic within the fascial plane. As a result, multiple injection sites may be required to achieve adequate coverage of the entire sternotomy incision.
Serratus anterior plane block
The serratus anterior plane block (SAPB) is another anterior approach targeting the lateral cutaneous branches of the intercostal nerves.
This block can be performed in two variations:
- Superficial SAPB between the serratus anterior and latissimus dorsi muscles
- Deep SAPB between the serratus anterior muscle and the ribs
Although these lateral nerve branches do not directly innervate the sternum, clinical reports have demonstrated analgesic benefit for sternotomy procedures. This effect is believed to result from the spread of local anesthetic to adjacent nerve branches.
Posterior fascial plane block techniques
Posterior thoracic blocks represent another group of fascial plane techniques used in pediatric cardiac anesthesia. These blocks target the intercostal nerves closer to their origin from the spinal cord.
Because the injection occurs near the dorsal and ventral rami, posterior blocks can potentially produce broader thoracic sensory coverage.
However, posterior blocks typically require lateral patient positioning, which limits their use after surgery, and repositioning critically ill patients may be impractical.
Erector spinae plane block
The erector spinae plane block (ESPB) has rapidly gained popularity in thoracic and cardiac anesthesia. In this technique, a local anesthetic is injected between the erector spinae muscle group and the transverse processes of the thoracic vertebrae.
The injected anesthetic spreads along the fascial plane and may reach both the dorsal and ventral rami of the spinal nerves.
Cadaver studies in neonates have demonstrated that injectate from an ESPB may extend into the paravertebral and epidural spaces, contributing to its broad analgesic effect.
The ESPB is considered technically straightforward and relatively safe because the needle trajectory remains distant from the pleura and major vascular structures.
Paravertebral block variants
Several newer regional techniques have been developed as alternatives to traditional thoracic paravertebral blocks. These include:
- Midpoint transverse process block
- Thoracic retrolaminar block
- Multiple-injection costotransverse block
These approaches aim to provide analgesic coverage similar to that of paravertebral blocks while avoiding direct needle placement within the paravertebral space.
Despite their theoretical advantages, current evidence does not clearly demonstrate improved safety compared with other fascial plane blocks.
Evidence supporting fascial plane blocks
A growing body of literature supports the use of fascial plane blocks for pediatric cardiac surgery. A narrative review identified 28 studies evaluating regional anesthesia techniques for children undergoing cardiac surgery via sternotomy, following an initial literature search that screened over 700 publications.
Across these studies, several consistent outcomes have been reported.
Reduced opioid consumption
Many randomized and observational studies demonstrate significant reductions in both intraoperative and postoperative opioid use when fascial plane blocks are included in multimodal analgesia protocols.
For example, randomized trials evaluating the transversus thoracic muscle plane block have reported substantial decreases in fentanyl requirements during the first 24 hours after surgery.
Similarly, erector spinae plane block studies show reduced morphine consumption and delayed time to rescue analgesia.
Improved pain control
Postoperative pain scores are another commonly reported outcome in clinical trials. Multiple studies demonstrate lower pain scores during the first 24 hours following surgery in patients receiving fascial plane blocks compared with standard analgesic regimens.
Although the magnitude of improvement varies between studies, the overall trend suggests meaningful analgesic benefit.
Enhanced recovery
Regional anesthesia techniques may also contribute to faster recovery following pediatric cardiac surgery.
Studies have reported improvements in several recovery metrics, including:
- Shorter time to extubation
- Reduced ICU length of stay
- Reduced hospital length of stay
These findings are particularly relevant to enhanced recovery after surgery (ERAS) pathways, which emphasize early extubation and rapid mobilization.
Safety considerations
Safety remains a central concern when introducing new regional anesthesia techniques in pediatric patients.
The available evidence suggests that fascial plane blocks have a favorable safety profile. Complications reported in the literature are rare and generally related to technical issues such as needle misplacement or loss of ultrasound visualization.
For example, one large retrospective study examining the transversus thoracic muscle plane block in nearly 200 pediatric patients reported only two complications: one pleural and pericardial puncture and one small subcutaneous hematoma.
Despite these reassuring results, clinicians must remain vigilant when performing deep anterior blocks due to their proximity to vital thoracic structures.
Limitations of current research
Although current evidence supports the use of fascial plane blocks in pediatric cardiac surgery, several limitations remain. Most published studies share several common characteristics:
- Small sample sizes, often fewer than 100 patients
- Single-center study designs
- Homogeneous patient populations with relatively simple congenital heart defects
These limitations reduce the generalizability of findings and highlight the need for larger multicenter trials.
Another challenge relates to outcome measurement. Pediatric pain assessment is inherently difficult, and pain scores are sometimes reported inconsistently or presented only graphically in published studies.
Additionally, many studies fail to account for pain originating from chest drains or other postoperative devices.
Future directions
Future research should focus on several key areas to improve the evidence base for regional anesthesia in pediatric cardiac surgery.
First, larger multicenter trials are needed to compare different fascial plane block techniques and determine the optimal approach for sternotomy analgesia.
Second, investigators should evaluate optimal local anesthetic dosing strategies, including the potential role of continuous catheter techniques for prolonged analgesia.
Third, studies should expand beyond relatively homogeneous patient populations to include neonates, patients with cyanotic congenital heart disease, and children undergoing more complex surgical procedures.
Finally, research should examine broader outcomes, including functional recovery, patient satisfaction, and long-term pain outcomes.
Conclusion
Fascial plane blocks represent a promising strategy for improving perioperative analgesia in pediatric cardiac surgery. By targeting the intercostal nerve branches responsible for sternotomy pain, these techniques can significantly reduce opioid requirements while maintaining effective pain control.
Evidence from randomized trials and observational studies suggests that fascial plane blocks may improve several clinically important outcomes, including pain scores, opioid consumption, time to extubation, and ICU length of stay.
Although further research is needed to define the optimal techniques and dosing strategies, current data support the integration of regional anesthesia into multimodal analgesia protocols for children undergoing cardiac surgery.
As ultrasound-guided regional anesthesia continues to evolve, fascial plane blocks are likely to play an increasingly important role in enhancing recovery and improving outcomes for pediatric cardiac patients.
For more information, refer to the full article in Anesthesia & Analgesia.
Russell GC, Einhorn LM. Regional Anesthesia With Fascial Plane Blocks for Pediatric Cardiac Surgery With Sternotomy A Narrative Review. Anesth Analg. 2026 Mar 1;142(3)507-517.
Download the Nerve Blocks App HERE for step-by-step guidance on fascial plane block techniques. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Module on NYSORA360!