Learning objectives
- Signs of amniotic fluid embolism (AFE)
- Management of AFE
Definition and mechanisms
- Amniotic fluid embolism (AFE) is one of the most catastrophic and life-threatening complications of pregnancy
- Occurs when amniotic fluid, fetal cells, hair, or other debris enters the maternal pulmonary circulation and causes cardiovascular collapse
- It is not a consequence of the “simple” mechanical respiratory obstruction, but a humoral effect causing anaphylactoid reactions or complement activation
- It can occur in:
- Healthy women during labor
- During cesarean section
- After abnormal vaginal delivery
- During the second trimester of pregnancy
- 48 hours post delivery
- During abortion
- After abdominal trauma
- During amnio-infusion
- Any breach of the barrier between maternal blood and amniotic fluid forces the entry of amniotic fluid into the systemic circulation and results in a physical obstruction of the pulmonary circulation
- The maternal prognosis after amniotic fluid embolism is very poor
Signs and symptoms
- Premonitory symptoms
- Acute dyspnea
- Sudden agitations
- Sudden chills, shivering, sweating
- Cough
- Anxiety
- Labored breathing
- Tachypnea
- Altered mental status, seizures, and coma
- A rapid decline in pulse oximetry values or sudden absence or decrease in end-tidal carbon dioxide
- Hypotension
- Cyanosis: ventilation-perfusion mismatching as a result of pulmonary vascular constriction
- Fetal bradycardia
- Encephalopathy
- Uterine atony
- Acute pulmonary hypertension
- Coagulopathy/ severe hemorrhage
Diagnosis
- Four criteria must be present to make the diagnosis of AFE:
- Acute hypotension or cardiac arrest
- Acute hypoxia
- Coagulopathy or severe hemorrhage in the absence of other explanations
- All of these occur during labor, cesarean delivery, dilatation, and evacuation, or within 30 min postpartum with no other explanation of findings
Course of AFE
- Typical (classic) with three phases
- Phase 1 respiratory and circulatory disorders
- Phase 2 coagulation disturbances of maternal hemostasis
- Phase 3 acute renal failure and acute respiratory distress syndrome (ARDS)
- Cardiopulmonary collapse
- Atypical
- Life-threatening hemorrhage due to disseminated intravascular coagulation (DIC)
Differential diagnosis
- Anaphylaxis
- Aortic dissection
- Cholesterol embolism
- Myocardial infarction
- Pulmonary embolism
- Septic shock
- Air embolism
- Transfusion reaction
- Eclamptic convulsions and coma
- Convulsion from the toxic reaction to local anesthetic drugs
- Aspiration of gastric contents
- Hemorrhagic shock in an obstetric patient
Risk factors or causes
- Unpredictable – unpreventable
Risk factors:
- Older maternal age
- Multiparity
- Intense contractions during labor
- Abdominal trauma
- Cesarean section
- Induction of labor
- Placenta previa
- Eclampsia
- Multiple pregnancies
- Tears in the uterus or cervix
- Early separation of the placenta from the uterus wall
- Fetal factors:
- Fetal distress
- Fetal death
- Male baby
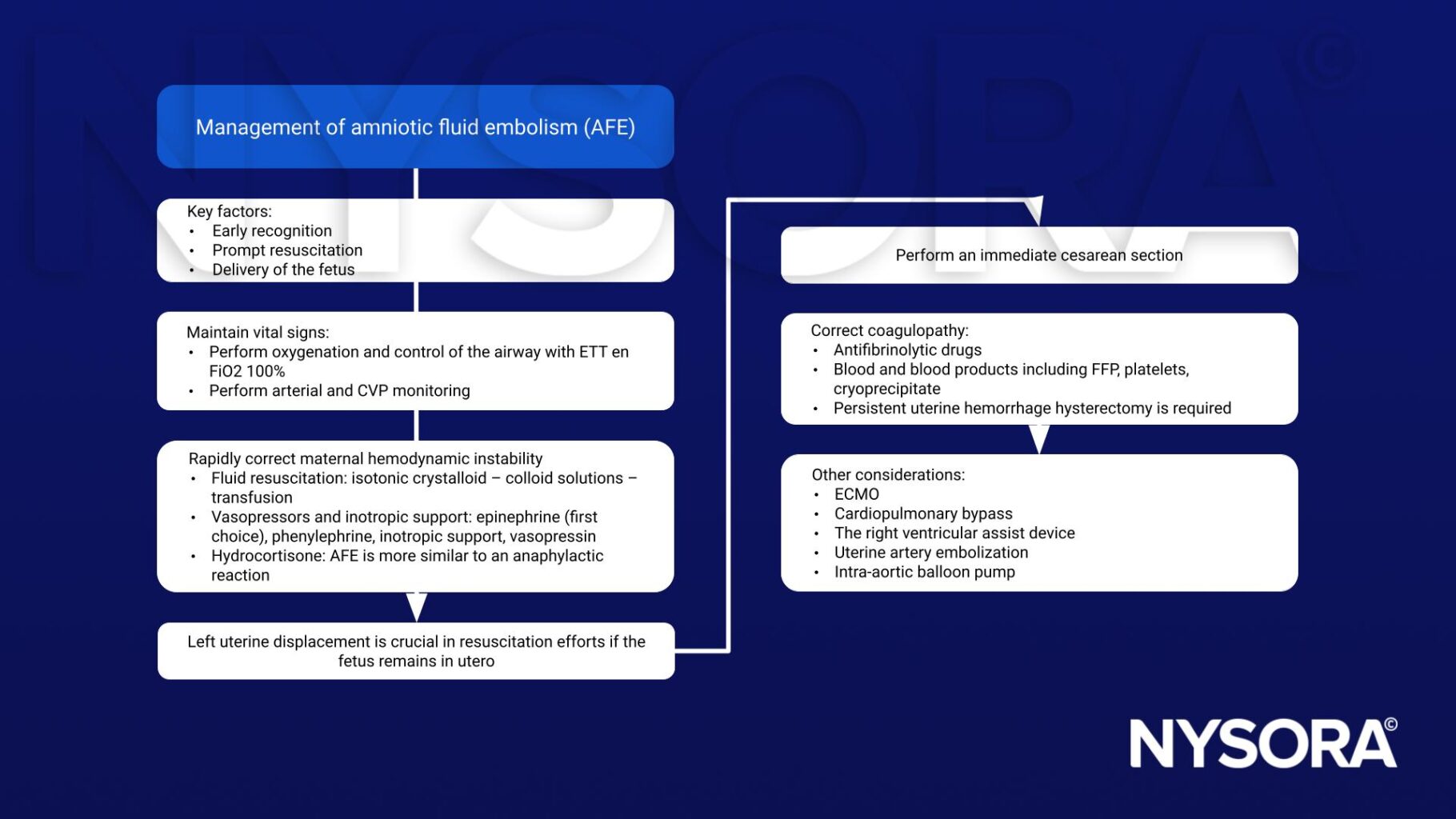
Management
Suggested reading
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Kaur K, Bhardwaj M, Kumar P, Singhal S, Singh T, Hooda S. Amniotic fluid embolism. J Anaesthesiol Clin Pharmacol. 2016;32(2):153-159.
Clinical updates
Neef et al. (Current Opinion in Anesthesiology, 2024) report that intraoperative cell salvage does not increase the risk of amniotic fluid embolism, despite historical concerns about fetal squamous cell contamination. Contemporary evidence supports the modern view of AFE as an anaphylactoid reaction rather than a mechanical embolic event, with no confirmed cases of iatrogenic AFE linked to cell salvage. These findings support the safe use of cell salvage during massive obstetric hemorrhage, including scenarios where AFE-associated coagulopathy is suspected.